In September 2011, a 55-year-old log truck driver was fatally injured when he was struck and crushed by logs being loaded by a grapple loader onto the trailer of his truck. The victim worked for a trucking company that had been contracted to haul logs by the company logging the site where the incident occurred. The loader operator worked for the logging company. Both were experienced in their fields, but had not worked together before beginning work at this site approximately one week prior to the incident.
All of the loads previously hauled from the site had been long logs. The logs to be loaded the morning of the incident were short logs. The previous night, the victim and his employer had extended the truck’s trailer and installed a rack with an extra set of bunks, also called a “turkey rack,” in order to haul the short logs. Bunks are lateral fixtures secured to a trailer that have vertical stakes at either end, and are used in pairs to contain logs during transport. The height of the bunk stakes on the victim’s trailer could be increased using metal extensions that must be manually lifted and secured into place. That night, the victim had left the bunk stake extensions lowered.
The morning of the incident, the loader operator arrived first to the jobsite, at approximately 5:00 a.m., and started to warm up the loader. It was still before dawn and darkness would have limited visibility. The victim arrived a short time later. While communicating by radio with the operator, the victim situated the trailer next to the loader, with the loader positioned on the passenger side of the truck near the rear of the trailer. The victim remained in the cab of the truck as the loader operator placed the first load of logs in the front set of bunks. The operator then turned the boom arm away from the truck and positioned the grapple to pick up another load of logs to place in the second set of bunks. As the loader operator swung the second load toward the rear bunks, he caught a glimpse of the victim’s orange high-visibility safety vest and realized that the victim was standing on the back of the trailer. The operator immediately reversed the direction of the load when he saw the victim, and two logs fell from the grapple. The loader operator stopped the equipment and went to the victim, who had been struck by the logs, and found him lying unconscious over the rear crossbar of the trailer. The loader operator could not lift the victim off of the trailer to begin CPR. He called 911 and tried to maintain the victim’s airway until emergency responders arrived. The victim had sustained crushing injuries and was pronounced dead at the scene. Emergency responders reported that the victim was wearing a long sleeved shirt over his safety vest. It is unknown why the victim left the cab, but investigators believe that he climbed onto the trailer to put up the stake extensions on the bunks that he had left lowered the night before.
To prevent similar incidents, Washington State Fatality Assessment and Control Evaluation (FACE) recommends that:
Communication Practices
Personal Protective Equipment
In September of 2011, The Washington State Division of Occupational Safety and Health (DOSH) notified the Washington State Fatality Assessment and Control Evaluation (FACE) program of the death of a 55-year-old log truck driver.
WA FACE investigators interviewed the owner of the trucking company where the victim had been employed. Documents reviewed during the course of this FACE investigation include the DOSH investigation file, sheriff’s office report, autopsy report, and death certificate. Owners and operators from other logging and trucking employers were also interviewed to provide additional information about common procedures and practices
The victim’s employer is a small trucking company that provides transport service to local logging operations, and also occasionally performs small logging operations. At the time of the incident, the company employed five full-time drivers and occasionally used contract drivers. The company has been in the trucking business since approximately 2000. They had been hired to haul logs by the general contractor logging the site. The employer had not been contracted by this logging company previously.
The employer has an accident prevention program (APP), as required by Washington State law, provides on-the job-training for newly hired employees, and conducts safety meetings with drivers approximately once a month. New hire training materials received by the victim included information about safe movement around machines. The training guide for truck drivers includes the directive:
The area behind the cab guard is considered a hazardous area. Do not enter the hazardous area until you have signaled the loader operator; and the operator has acknowledged it is safe to enter the hazardous area and you have checked the load for unstable logs. After leaving the hazardous area and you are positioned “in the clear”, again signal the operator.
One of the company’s general safety rules states “Do not approach a machine’s working circle until the operator has acknowledged that it is safe to do so.”
The victim was a 55-year-old log truck driver who had been employed by the trucking company for several years. He had been driving log trucks for over 15 years. He had experience hauling both long logs and short logs, and had worked with many loader operators over the years. According to the employer and other employees of the trucking company, the driver was known for always wearing proper PPE, including his high-visibility safety vest.
The loader operator had been a logger and equipment operator for over 30 years. At the time of the incident, he had worked for the company logging the site off and on for approximately 4-5 years. A foreman who had previously worked with the operator in the past remembered him as a “very good operator” who did not put productivity before safety.
The victim was very accustomed to driving the log truck, and had driven it exclusively for the previous three years. The employer had purchased the truck used with the operator’s manual. The night before the incident, the victim and the employer extended the trailer and equipped it with a rack with two extra bunks, known as a “turkey rack” (Photo 1), for the purpose of hauling two loads of short logs (typically 12-24 feet long) at one time. Bunks are lateral fixtures secured to a trailer that have vertical stakes at either end, and are used in pairs to contain logs during transport. On this trailer, the height of each vertical bunk stake could be increased by manually raising an extension rod and securing it with a metal pin. The bunk stake extensions were left lowered at the time the turkey rack was loaded into the truck.
The loader used was a Komatsu PC 200 LC-5L tracked log loader with a grapple, also known as a grapple loader (Photo 2). A post-incident safety inspection by an independent party showed the machine to be in good working condition, with all lights functional and no bleed off from cylinders with a suspended load. There were three lights on the front of the cab and one on the rear.
The incident occurred shortly before sunrise, and it would most likely have been too dark at that time to carry out normal operations without the use of artificial illumination. The weather that morning was cool, dry, and calm.
The victim’s employer had been contracted by a logging company to haul logs from the incident site. The loader operator worked for the logging company. The victim and the loader operator had been working together at the site for approximately one week before the incident, but had not worked together prior to this job.
The Komatsu PC200 LC-5l grapple loader had been moved to the site by the logging company eight days earlier, and the loader operator and his employer had reviewed its controls and operation at that time.
The trucking company began hauling logs from the site the next day. Until the time of the incident, all of the logs that the victim had transported from the site had been “long logs” which had been loaded onto trailers of standard configuration. On the day of the incident, only one truck would be needed to haul the remaining “short logs” from the site, according to the victim’s employer.
On the evening before the incident, the victim and his employer had configured the truck for hauling short logs by extending the trailer and adding a rack with a second set of bunks, or “turkey rack.” That night, the metal extension rods that are used to increase the height of the bunk stakes were left lowered.
On the morning of the incident, the loader operator arrived at the worksite before the victim, at approximately 5:00 a.m. He proceeded to warm up the loader. The victim drove the truck onto the site shortly after. The victim’s intended task that morning was to transport loads of “short logs” (12-24 feet in length) from the site. It was still before sunrise. The landing at the site was open and level. The victim backed the log truck into position with the loader located between the log deck and the rear of the trailer on the passenger side of the truck (see Figure 1). There was another stack of logs in front of the loader. In this position, when lifting logs with the grapple in line with the tracks, the cab of the loader would be faced away from the cab of the truck. The victim and the loader operator were reportedly in radio contact during the configuration process.
The victim was in the cab of the truck at approximately 5:15 a.m. when the loader operator placed the first load of logs in the bunks at the front of the trailer. The loader operator then turned the cab and boom arm away from the trailer and picked up the next two logs to place in the rear bunks. As the loader operator was bringing the second pair of logs around toward the rear of the trailer, he suddenly caught sight of the victim’s orange safety vest and realized that he was standing on the back of the trailer. The loader operator immediately reversed direction of the load, and both logs fell from the grapple and landed on the ground behind the trailer. The loader operator left the cab and found the victim lying unconscious over the bar of the rear bunk. He had been struck by the logs either as they were being swung toward the bunk or as they fell.
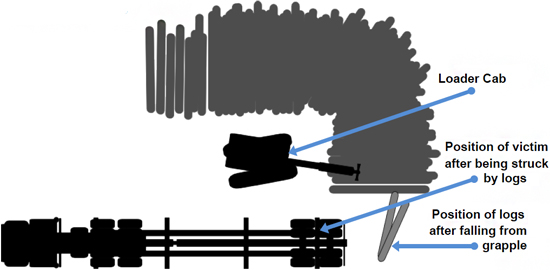
Figure 1: Incident site
The loader operator was trained in first aid and CPR, but was not able to lift the victim down from the trailer alone. He contacted 911 and attempted to maintain an airway for the victim while waiting for emergency responders. The victim was declared dead at the scene. Emergency responders reported that the victim was wearing a long-sleeved shirt over his high-visibility safety vest.
The medical examiner attributed the death to a crush injury of the left pelvis, with bilateral rib fractures contributing to death. Postmortem toxicology testing was negative for drugs and alcohol.
Recommendation 1: Employers should train log truck drivers to always establish and confirm visual or radio communication with the loader operator before leaving the cab of the truck during loading procedures.
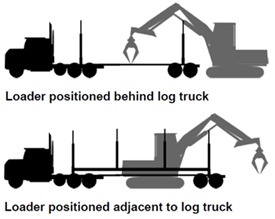
Figure 2: Loader positions
Discussion: It is standard practice for log truck drivers and loader operators to remain in contact, either by radio or hand signals, during loading procedures. Communication is necessary to configure the truck and trailer for loading, and to maintain proper weight distribution on the trailer
It is impossible to know why the victim did not convey his intention to leave the cab to the loader operator on the morning of the incident. Despite his training, the victim may have simply overlooked this critical step for any number of reasons. After the original communication between the victim and the operator, it is possible that a technical issue occurred: the radio channel was accidently changed, the volume was turned down, or the squelch was not working properly. The victim may have thought that he was communicating with the loader operator, but without waiting for confirmation, he would not have known that his intention to go to the rear of the trailer went unheard.
Employers should train employees to wait for affirmative confirmation that the loader operator has received their communication before leaving the safety of the cab. In addition, employers should consistently emphasize the importance of communication at safety meetings and review communication procedures frequently.
The victim’s employer now trains his drivers that they must get a confirmation response from the loader operator before going behind the cab guard for any reason, such as when they pull the bunk pin on the trailer.
Recommendation 2: Employers should train loader operators to verify by sight or radio contact that the driver is in the clear before loading.

Photo 3: View from forward facing window of loader cab
Discussion: Often during loading, the loader will be positioned behind the trailer facing the truck cab; the employer indicated that this was the typical arrangement in his experience. In this position, the operator has a relatively unobstructed view of the trailer and cab in most positions when rotating the loader, and would be more likely to see if the driver exits the cab. On the morning of the incident, the landing was configured in such a way that the loader was located adjacent to the trailer facing away from the cab of the truck (Figure 2).

Photo 4: View from right side window of loader cab,
with grapple resting on front of log deck
In this location, boom arm movement occurred between the loader cab and the trailer. It is likely that as the loader operator was lifting the second load of logs off the deck and swinging them toward the rear bunks, his view of the trailer was partially obscured by the arm of the boom (Photos 3 & 4), and he would not have been able to see the victim on the trailer near the rear passenger side bunk stake until he had almost fully rotated back toward the trailer (Photo 5).
Had the loader operator been able to better see the trailer during the movement of the second load, he might have seen that the victim had left the cab and climbed onto the trailer, but the position of the loader allowed for blind spots. In situations such as this, where visibility of the truck cab or trailer is obstructed or reduced, employers should instruct loader operators to take the extra step of verifying the driver’s position prior to loading.

Photo 5: Approximate location of victim on trailer when struck by logs
Recommendation 3: Employers should ensure that when employees are working with a new company or crew member, or when conditions or procedures change, the intended loading process is reviewed before loading begins.
Discussion: The victim and the loader operator were both very experienced in their fields. However, the companies that employed them had only been working together for about a week at the time of the incident. The victim’s employer indicated that safety information between logging and trucking companies is usually implied, not explicit. In this situation, expectations of standard operating procedures for loading short logs on a turkey rack may have differed between companies.
The victim’s employer stated that after the first load of logs had been loaded in the front bunks, the victim’s standard procedure would have been to exit the cab to raise the bunk stake extensions on the trailer and collect a load ticket from the operator before the rest of the trailer was loaded. Other drivers and operators that FACE investigators spoke with use procedures in which the ticket is collected after the trailer is fully loaded.
Although the victim and operator had worked together in previous days hauling long logs, they may have had different expectations of the order of procedures for short logs. The loader operator’s expectation was that the victim would remain in the cab as he immediately loaded a second set of logs onto the rear bunks. The victim may have left the cab under the false assumption that he and the operator had a common understanding of the next steps in the sequence. A pre-loading procedure review could have eliminated any confusion about the intended sequence of events.
Recommendation 4: Employers should provide log truck drivers with appropriate high-visibility safety vests and train them to ensure that they are worn in an effective manner.
Discussion: The victim’s employer and co-workers reported that the victim was known for consistently wearing his safety vest. On the morning of the incident, the victim wore his safety vest, but EMS responders at the scene reported that he wore a long-sleeved shirt over the vest. With the front of the shirt unbuttoned the vest would only have been visible at certain angles. Employers should provide high-visibility safety vests and train employees in their effective use, give frequent reminders at safety meetings, and ensure proper use through spot checks. Correct use of high-visibility gear is especially important when working in dark conditions where visibility is already limited. The loader operator stated that it was the reflection from the safety vest that first caught his eye and signaled that the victim was on the trailer. It is possible that the loader operator may have seen the victim sooner had he not been wearing a shirt covering the back of his safety vest.
This report was reviewed by stakeholders from labor and business communities and various Washington State and Federal worker safety agencies. Though we are unable to acknowledge specific individuals for their contributions to this report, we would like to recognize the following for their help and support of the FACE mission and objectives:
Todd Schoonover has a PhD in Industrial Hygiene from the University of Illinois at Chicago. He is a Certified Industrial Hygienist (CIH) and Certified Safety Professional (CSP). Todd is currently the Principal Investigator for the WA FACE program.
Randy Clark has a BA from The Evergreen State College. He is a Safety and Health Specialist with the WA FACE program.
Christina Rappin has a BAS from The Evergreen State College. She is a Research Investigator with the WA FACE program.
Washington State FACE Program Information
The Washington State Fatality Assessment and Control (WA FACE) program is one of many workplace health and safety programs administered by the Washington State Department of Labor & Industries’ Safety & Health & Research for Prevention (SHARP) program. Under a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH grant# 5 U60 OH008487-09), WA FACE collects information on occupational fatalities in WA State and targets specific types of fatalities for evaluation. WA FACE investigators evaluate information from multiple sources. Findings are summarized in narrative reports that include recommendations for preventing similar events in the future. These recommendations are distributed to employers, workers, and other organizations interested in promoting workplace safety. NIOSH-funded, state-based FACE programs include: California, Iowa, Kentucky, Massachusetts, Michigan, New Jersey, New York, Oregon, and Washington. WA FACE does not determine fault or legal liability associated with a fatal incident. Names of employers, victims and/or witnesses are not included in written investigative reports or other databases to protect the confidentiality of those who voluntarily participate in the program.
Additional information regarding the WA FACE program can be obtained from:
Washington State FACE Program
www.lni.wa.gov/safety/research/face/
PO Box 44330
Olympia, WA 98504-4330
1-888-667-4277
Publication #: 11WA03301| May 15, 2015
Disclaimer and Reproduction Information: Information in NASD does not represent NIOSH policy. Information included in NASD appears by permission of the author and/or copyright holder. More
