Acknowledgements
Conference Directors
Faculty
Executive Summary
Background
Conference Format
1. The Scope of the Problem of Stooped and Squatting Postures in the Workplace
2. Scientific Basis for Understanding the Effects of Stooped and Squatting Postures in the Workplace
3. Controlling Stooped and Squatting Postures in the Workplace
4. Suggestions for improving Prevention of Musculoskeletal Disorders Caused by Stooped, Squatting or Kneeling Postures
References
Stooped postures have probably been with us since the first human ancestors began walking upright. In the modern world, it might appear that stooped postures are confined to work in developing countries or less mechanized workplaces. However, nothing could be further from the truth. Stooped postures are commonly found in agricultural, construction, mining, and other workplaces all around the world. Further, work requiring stooped postures is strongly associated with high incidence of low back disorders (LBDs). Nonetheless, the terms “stooped” or “squatting” postures are not commonly found in ergonomics studies or literature. These facts taken together led to the questions that stimulated this conference: (1) what do we know about the scope of stooped, kneeling and squatting postures in the workplace; (2) what scientific basis is there for understanding the effects of these postures; and (3) what do we know about strategies for controlling stooped postures?
Speakers at this conference made clear that the problem of stooped and squatting postures in the workplace is global in scope and widespread in many industries. Further, evidence presented made clear that stooped postures are commonly associated with work that has a high incidence of LBDs. Nonetheless, stooped postures have been little studied as a primary risk factor for LBDs. Most attention on risk factors for LBDs has been focused on manual materials handling and whole-body vibration. Stoop (sustained bending of the spine) has been largely neglected. In part, this may be due to the lack of an accepted definition of stooped or squatting postures. As this conference ended, we accepted the following as initial working descriptions: a stooped posture can be defined as “bent forward and down from the waist and/or mid-back while maintaining relatively straight legs”; squatting can be described as a “bending of EXECUTIVE SUMMARY the knees so that the buttocks rest on or near the heels”.
The full scope of the problem is not well reflected in occupational injury data because current reporting methods do not examine the relatedness of an injury to stooped and squatting work postures. Workers’ compensation programs focus more on delivering benefits than prevention efforts, and claims data collection is driven by injury (an ‘event’) rather than cumulative trauma. Reducing the incidence of work-related LBDs in these jobs will require a new focus on identifying and describing stooped and squatting postures as specific LBD risk factors in the workplace.
Biomechanical research shows that high spinal compression forces occur in stooped postures, and that sustained or repeated flexion of the spine may disturb the neuromuscular stability of the lower back and increase the risk of fatigue, leaving the back more vulnerable to injury. What is missing (as is the case with many ergonomics risk factors) is definitive etiology demonstrating the causal role and mechanisms linking stooped postures with MSDs.
While there is considerable epidemiological evidence associating working in stooped, kneeling and squatting postures to LBDs, it is mostly focused on those postures in combination with other risk factors such as bending or twisting or heavy loads. The literature combining stooped, squatting or kneeling postures with load handling shows rapid and severe spinal damage. There is much less in the literature regarding the health effects of these postures in an unloaded situation.
Kneeling and squatting are often seen as alternatives to stooping as a way to work at low levels without bending the back as much. In agriculture and construction, workers often resort to stooping because it demands less energy expenditure than the alternatives, and they can exert higher force and have increased mobility than when kneeling or squatting. There is good biomechanical reason to view these postures as significant contributors to MSDs of the knee and low back. There are generally few studies of knee injuries associated with these postures, and conclusive, causal studies are still lacking. Job improvement efforts should target reduction of existing risk factors, while avoiding increased risk to other regions of the body.
Determining which controls are available as interventions to the problem of stooped work is challenging for the industries of concern, especially agriculture, construction, and mining, because they have tremendous variation in their workplace environments. Four classes of interventions were discussed at the Conference, and successful interventions in all these areas were presented:
- Reduce or Eliminate the Need to Stoop or Squat
(e.g., raised planting beds, portable tables or carts,
lifting aids and handles)
- Mechanical Worker Protection or Worker Aids
(e.g., devices to facilitate kneeling, prone workstations,
and load transfer devices)
- Mechanical Assists to Allow the Employee to Work in
a Standing Position
(e.g., tool extensions, mechanical harvesting, wheeled
roofing equipment for tear-off, fastening, and
bitumen application.)
- Administrative Controls
(e.g., programmed breaks, reducing the number of
working hours, or hiring more workers during peak
periods to reduce the demands on the individual
worker).
However, intervention experts were unanimous in noting that interventions must be task- and situation-specific to be both adoptable and effective. This means that few interventions can be expected to travel un-adapted between jobs or tasks.
In order to improve our understanding of the relationship of stooped, squatting and kneeling postures and MSDs and their prevention we must increase and improve research focused on these risk factors. A necessary first step will require differentiation by the research community between stooped posture and stooped work. This may be achieved by determining at what exposure level assuming a flexed posture becomes ‘stooped work’, and establishing a consensus definition of stooped work (e.g., work below knees > 40% of time).
Secondly, there is a need to develop practical and objective measures of exposure to stooped work (degree of bending, duration, frequency) and refine the epidemiological case definition of outcome (symptoms, physical findings, diagnoses) for a deeper focus on the effects of stooped work.
To seriously begin to improve our understanding of the etiology and causal relationship between stooped and squatting postures and MSDs we need to increase our understanding of the biomechanics of the spine and the lower extremities in these positions. There is a need for research studies designed to evaluate the effects of these postures on tissue responses under various conditions and loading patterns. Research is required to understand how the intervertebral disc, the meniscus of the knee, and other passive tissues respond to repetitive versus static loading. Such research may point the way to understanding the relationship of degrees of postural stress and disease and, similarly, how much postural relief is needed or useful in preventing disease. Epidemiology and biomechanics provide much of the basis for understanding the effects of working in stooped and squatting postures, and the knowledge gained from such study needs to be incorporated into the case definition of stooped work, and in job design criteria that take into account the tissue fatigue generated by static postures.
Finally, there is need for an improved system of intervention research that both disseminates the evaluation of alternative strategic approaches in different workplaces and supports the development of workplace specific adaptations of known approaches. Interventions that are not both acceptable to workers and employers and that fit the work system without serious detriment to productivity will not be widely adopted. Development of such interventions is neither an automatic nor guaranteed result of publication of research results or successful demonstrations in other industries.
SUGGESTIONS FOR IMPROVING PREVENTION OF MUSCULOSKELETAL DISORDERS CAUSED BY STOOPING, SQUATTING OR KNEELING POSTURES
SUGGESTIONS FOR ASSESSING HIGH RISK JOBS
- Evaluate the effectiveness of different methods of risk assessment with attention to predictive ability and field utility.
SUGGESTIONS FOR SURVEILLANCE RESEARCH
- Develop a national registry of musculoskeletal hazards and health outcomes.
- Add supplements to existing surveillance systems for stooped, squatting, and kneeling postures.
- Conduct surveys in high risk industries (agriculture, construction, mining).
- Determine the number of workers exposed and what jobs they are doing.
- Record the exposure in identified jobs: time in stooped and squatting, by ‘zones’ of mild, moderate, and severe positions.
- Identify the specific job or task elements requiring stooped postures, and why.
- Conduct cross-sectional and longitudinal studies to develop and validate a list of high risk jobs and significant health outcomes.
SUGGESTIONS FOR INTERVENTION RESEARCH
- Develop new partnerships with agencies, academia and industry to support intervention research focused on stooped, squatting, and kneeling work, including national and regional partnerships focused on industry- or task-specific applications.
- Increase the number and range of intervention research underway.
- Encourage higher-quality intervention evaluations using randomized trials, quasiexperimental designs and blended evaluations.
- Document and broaden the dissemination of successful/proven interventions.
SUGGESTIONS FOR ETIOLOGICAL RESEARCH
- Conduct studies to improve understanding of specific biomechanical stresses and MSD development during stooped, squatting and kneeling postures.
- Develop and evaluate improved standards and methods for assessing exposure, health outcomes and other etiological factors for stooped, squatting and kneeling work.
- Conduct population, clinical and laboratory studies to evaluate the short term impacts of different types of exposure to working in stooped, squatting or kneeling postures on MSD development and early indicators of such disorders.
- Conduct population, clinical and laboratory studies to evaluate the long term impacts of different types of exposure to working in stooped, squatting or kneeling postures on MSD development and early indicators of such disorders.
Work-related musculoskeletal disorders (WMSDs) are one of the greatest occupational health concerns today. Of the many types of WMSDs, low back disorders (LBDs) are the most prevalent and by themselves constitute a major health and socioeconomic problem. Decades of research has identified certain physical workplace factors that increase the risk for LBDs. A review by the National Institute for Occupational Safety and Health (NIOSH) of epidemiological studies related to MSDs in the workplace (NIOSH, 1997) found evidence for an association between LBDs and the following workplace factors: 1) heavy physical work, 2) lifting and forceful movements, (3) bending and twisting (awkward postures), and 4) whole-body vibration. While much attention has been focused on manual materials handling (MMH), lifting, and whole-body vibration, the LBD risk factor of sustained bent and twisted positions of the spine has been relatively neglected. Static forward-bent postures, often associated with working at or near ground level, are commonly observed in agriculture, construction, mining, and certain other industries that have a high incidence of LBDs. Reducing the incidence of occupational LBDs in these jobs requires a new focus on the problem of stooped and squatting postures in the workplace.
In over a decade of ergonomics field research in California agriculture, the staff of the UC Agricultural Ergonomics Research Center (UC AERC) identified stooped postures as one of three virtually endemic risk factors in California agriculture for which few proven interventions were available. Stooped postures are common in agriculture, BACKGROUND construction, mining and other occupations in highly industrialized societies and are more commonplace in less mechanized regions of the world. In order to learn more about the scope of the problem, the scientific basis for the role of stooped and squatting postures in WMSD development, and potential interventions a conference of experts was planned with funding from the National Institute for Occupational Safety and health (NIOSH).
On July 29-30, 2004, national and international experts in occupational safety and health convened in Oakland, California for the conference
Stooped Postures in the Workplace. The conference was jointly sponsored by the UC AERC, NIOSH, the University of California Center for Occupational and Environmental Health, the Center to Protect Workers’ Rights, and the California State Compensation Insurance Fund. To the best of our knowledge, this is the first conference to focus exclusively on the effects of stooped and squatting postures on work related musculoskeletal disorders and on related ergonomic intervention efforts. The objectives of the conference were to (1) identify and summarize available information on the ergonomics, etiology, and health effects of stooped postures; (2) identify and describe alternative strategies for eliminating or reducing the need for stooped postures in workplaces and for reducing worker exposures; and (3) facilitate sharing of information on these issues, and providing a basis for improving preventive strategies. This report summarizes the key findings from the two days of presentations and discussions.
The conference was organized into three sessions, each consisting of presentations and discussions focused on one of three main areas of interest:
- The Scope of the Problem of Stooped and Squatting Postures in the
Workplace
- Scientific Basis for Understanding the Effects of Stooped and Squatting
Postures in the Workplace
- Controlling Stooped and Squatting Postures in the Workplace
Each session consisted of a minimum of three presentations focused on the categorical topic. After each presentation, a brief period was allowed for questions from the audience. Upon the conclusion of all presentations for the session, a panel discussion was conducted to clarify and expand upon concepts that emerged during the course of the session. Owing to the nature of interdisciplinary research, many presenters provided content within their scheduled session that pertained to one or both of the other sessions. In order to maximize the breadth and depth of the knowledge provided by this conference, the authors of these proceedings Wickstrom G, Hanninen K, Mattsson T, Niskanen T, Riihimaki H, Waris P, Zitting A. 1983. Knee degeneration in concrete reinforcement workers. Brit J Ind Med 40:216-219. have chosen to organize this document based on how the content of the presented material addresses the three main categories of interest, rather than by the specific session in which it was presented.
Thomas Waters – Stooping at Work:
A Risk Factor for Low Back Pain?
(U.S. Perspective)
Adarsh Kumar – Stooped and Squatting
Posture Problems in Agriculture:
International Perspective (India)
Peter Lundqvist – The Scope of the
Problem of Stooped and Squatting
Postures in the Workplace, International
Perspectives: (Sweden)
R.J. Banks – Related Injury Incidence in
California
John Rosecrance – What Can
Epidemiology Tell Us?
William Marras – Biomechanics of Low
Back Disorders
Sean Gallagher – Capabilities and Costs
of Working in the Stooping Posture
Willette “Billy” Gibbons – Interventions
for Stooping/Bending Postures in
Construction
Laura Welch – Bend Your Knees, Not
Your Back: Work Accommodation for
Stooped Postures among Construction
Workers
Suzanne Rodgers – What Should We
Consider in Evaluating Workplace
Interventions?
Julia Faucett – Rest and Recovery Breaks
as Interventions
John Miles – Agricultural Interventions
in the U.S.
Peter Lundqvist – Agricultural
Interventions in Sweden
Fadi Fathallah – Risk Factor Control for
Stooped Postures in Agriculture
Robert Meyer – Research and Recent
Ergonomic Developments in Prone
Posture Workstations for Agriculture
Ira Janowitz – Conference Summation
The association between stooped work and low back disorders is not a new discovery. In 1713, Bernardino Ramazzini noted the bent-forward postures of porters who loaded and unloaded cargo ships in Venice and other seaports. In De Morbis Artificum Diatriba, he wrote that “All porters become in time round-shouldered, because the dorsal vertebral are constantly bent forward and become set in that position” (Ramazzini, 1713).
A focus on stooped and squatting postures in the contemporary workplace begins with an understanding of the national and international significance of the problem. Tom Waters, of the National Institute of Occupational Safety and Health (NIOSH), presented a perspective of the problem of occupational low back disorders (LBDs) in the United States and its relationship to work in stooped and squatting postures. The annual incidence of back pain in the United States is estimated to be 10-17% of the population, and lifetime incidence may be as high as 80% of the population. Occupational LBDs account for 34% of the cost of all work-related injuries and illnesses, with its estimated costs to be US$49 billion annually in 1992 (Leigh et al., 1997). In current dollars, the cost would exceed $100 billion per year! For many industries, LBD is their most significant occupational health problem. Research into the causes of LBDs has established its job-related physical risk factors: manual material handling (MMH), repetitive movements, and awkward posture (bending, twisting, and reaching). Focusing on the risk factor of posture, most researchers agree that working in a stooped posture for extended periods increases the risk of low back disorders. At the national level, NIOSH is concerned about the effects of prolonged stooping and squatting at work and is interested in research studies designed to evaluate the effects of stooped postures on the risk of LBDs, and on targeted ergonomics interventions that may be effective in reducing this risk.
Proportion of Individuals with WMSDs in the Low Back the Last 12 Months
| |
work in twisted position |
| lifting 15-25 kg several times |
|
men |
women |
|
≥1/4 work shift |
<1/4 work shift |
≥1/4 work shift |
<1/4 work shift |
| every day |
18.6 |
11.6 |
21.3 |
11.0 |
| every week |
12.1 |
4.8 |
13.0 |
5.6 |
|
|
For an international perspective on the problem of stooped and squatting postures in the workplace, the conference was pleased to welcome Peter Lundqvist of the Swedish University of Agricultural Sciences and Adarsh Kumar of the Indian Agricultural Research Institute. Dr. Lundqvist summarized the problem of WMSDs in Sweden, an industrialized nation with an economy similar to many other Western European nations. More than 40% of all reported acute and non-acute work injuries in Sweden are musculoskeletal in nature. Swedish occupational injury statistics show high rates of MSDs in jobs with frequent heavy lifting and tasks requiring repetitive work. For individuals reporting LBDs in the past 12 months, the injury rates approximately double with work in a twisted position more than 25% of the work shift, or when exposed to heavy lifting on a daily (vs. weekly) basis. The injury rates double again when heavy lifting is combined with a twisted posture.
High rates of WMSDs and exposure to awkward postures have been identified in Swedish agriculture. Mail survey results from Swedish agricultural workers reported a high frequency of pain and discomfort in shoulders, elbows, low back, hips and knees, and studies in the dairy industry have determined that awkward postures and high mechanical loads are common, especially in milking operations. Further development in addressing these problems is needed, with a focus on ergonomics research and solutions through international collaboration.
Perhaps nowhere is the problem of stooped and squatting postures of greater magnitude than in developing countries such as India. As presented by Dr. Kumar, India is one of the world’s largest agricultural economies and has the second largest agricultural workforce, with 260 million workers. The number of person-hours expended in crop production in India is measured in billions; for example, in rice alone the number is 44 billion person-hours per year. Although a few operations are partially mechanized, most agricultural operations are completely dependent on manual labor, with 800 million hand tools in use. Energy expenditures of common agricultural tasks using hand tools range from 13 to 40 kilojoules per minute; most of these exceed US NIOSH recommendations for exertions of more than one hour per day.
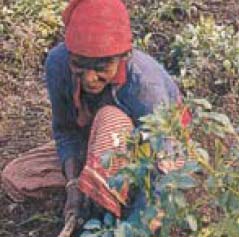
Observational studies of Indian agricultural workers identify frequent heavy lifting, forceful exertions, and work in stooped and squatting postures as key risk factors. Agricultural work in India is highly varied due to the small size of farms. The tasks performed, tools used, and work posture vary by crop and time of year, making it difficult to link cause and effect for MSDs over time. Weeding, harvesting, and cleaning crops are all commonly performed in either stooped or squatting postures. Even draft animal-assisted tasks can involve prolonged trunk flexion, as illustrated by cultivation, sowing, and fertilizer application using camels and bullocks. In plowing paddy fields, a stooped posture is maintained while simultaneously exerting substantial force to maintain the depth of the furrow (De and Sen, 1986). Required force, energy expenditure, and worker discomfort all varied with plow handle height (Gite, 1991). In semi-mechanized fodder cutting and threshing operations, feeding the machine often involves sustained stooping or squatting due to the design of the equipment.
- Agriculture
- Construction and utilities
- Mining
- Manufacturing
- Healthcare (nursing, dental & other patient care)
- Professional cleaning and custodial work
- Foodservice
- Retail sales
- Education and childcare
|
|
Potato harvesting in India |
Health care |
Having established a global significance, the Conference’s examination of the scope of the problem of stooped and squatting postures in the workplace continued by considering how they can be defined and in which jobs they are most prevalent.
During the conference, several researchers presented a definition of stooped posture that drew from literal definitions of “stooping” and/or their own observations of stooped or squatting posture work. A common definition of a stooped posture was “bent forward and down at the waist and/or mid-back while maintaining straight legs.” A squatting posture can be described as a “bending of the knees so that the buttocks rest on or near the heels”. Certain workplace characteristics were linked with these definitions, such as 1) low working height “at or near ground level” or “at or below knee height”; 2) little or no external weight is supported or lifted; and 3) duration of the posture is “sustained” or “maintained for a long period of time”. These additions to the definitions of stooped and squatting postures stem from the lack of a much-needed delineation between the
posture and the
work. The multiple definitions of stooped and squatting postures emphasize the need for clear definitions of stooped, squatting, and/or kneeling work when developing exposure measures or performing job analysis. In many studies and ergonomics checklists, the term “awkward posture” is used broadly to include squatting, stooping, and trunk bending in various directions.
The second element of defining stooped and squatting postures in the workplace is determining which jobs have the highest percent of time spent in stooped and squatting postures. Though these postures are observed in all lines of work, there are certain industries and jobs in which stooped and/or squatting postures predominate. A search of the 2004-2005 U.S. Department of Labor Occupational Outlook Handbook (BLS, 2004) for “stoop” or “stooping” among working conditions for a wide range of occupations returned results for agriculture, construction, mining, physical and occupational therapists, and a variety of repair workers. In addition, several presenters at this Conference illustrated jobs in manufacturing, professional cleaning, retail stores, food service, nursing, medical and dental, and teaching that have frequent stooped and/or squatting postures. Although stooped and squatting work is most prevalent in agriculture, construction, and mining, it is important to recognize that these risks are present in many other professions, including some that are not usually considered to be physically demanding.
Having defined what stooped and squatting postures are and where they are most often observed in the workplace, the final step in investigating the scope of the problem is determining the information relating to working in stooped and squatting postures that is provided by surveillance of workplace injuries. Surveillance of occupational injury takes place at many levels, from the job, employer, union, and insurer, up to state and national levels. It is dependent on both a system of injury reporting, and on the incentives and disincentives for workers to report injuries. In many countries, the lack of affordable health care and compensation provides little incentive for injury reporting. There seems to be an acceptance of high rates of MSDs in many industries throughout the world, including agriculture and construction, and low back and knee pain are often considered ‘normal’. Reporting of MSDs by the rural population is very limited, although the actual incidence of MSDs may be extremely high. An epidemiological study of nine villages in Northern India (Kumar et al., 1999) indicated that, in a combined population of 30,000, only 258 cases of musculoskeletal problems were formally reported in one year. However, medical and MRI examinations of a sample of agricultural workers from the region revealed high levels of abnormal objective findings. Such levels of spinal abnormalities are much higher than those previously reported in the literature, and suggest that the work activities of this population contributed to degeneration of the spine. Participants who drove tractors complained of more low back pain than agricultural workers who did not, but no objective differences were found between the two groups.
These findings support the view that, although a low rate of back pain was reported, agricultural workers in India (and perhaps in other developing countries) are at high risk of developing LBDs. The low level of availability of affordable health care and compensation benefits in this population may be among the reasons for this discrepancy. The limited means to treat and accommodate injured workers underscores the need for international, interdisciplinary research into problem areas such as working in stooped and squatting postures.
Similar problems extend to the immigrant labor force of industrialized nations. However, most industrialized nations, especially those with the largest economies, have an injury reporting system that is capable of tracking MSDs and LBDs in the workplace. Such nations also have workers’ compensation programs through which insurance claim data are assembled and analyzed. Nevertheless, significant disincentives may exist in situations where employees fear job loss or other adverse consequences for formally reporting pain or injury, and significant under-reporting is found even in highly industrialized societies (Morse, 2001).
In the United States, the two most available sources of injury data are employer OSHA logs and insurance claim records. Looking at these data sources, one might expect to see high rates of MSDs and LBDs in jobs with the highest exposure to stooped and/or squatting postures, which is generally confirmed by injury reports and claims experience. However, these two sources of injury data are not specific enough to track injuries related to working in stooped and squatting postures. In this Conference, examination of the deficiencies of employer injury logs and insurance claim records underscores the need for improvements in surveillance of injuries related to working in stooped and squatting postures.
In the United States, employers are required by law to record worker injuries on injury log forms and submit these records to state and federal OSHA agencies. However, stooping is not reported as a work activity on any of the OSHA injury log forms. The injury log asks for such information as the date of injury, where the ‘event’ occurred, a description of the injury or illness, and the object/substance that directly injured or made the person ill [California OSHA Form 300 (Rev. 4/2004)]. There is a focus on what happened just before the injury occurred, with no inquiry regarding the worker’s normal daily work activities. For stooping-related injuries to be identified from these data, the forms would need to be modified to gather information indicating whether his/her usual work activities include known LBD and/or knee injury risk factors, such as working in stooped or squatting postures.
Insurance claim data do not provide sufficient links between working in stooped and squatting postures and workers’ injuries. R.J. Banks, the Ergonomics Services Supervisor of the California State Compensation Insurance Fund (SCIF) presented an analysis of related injury incidence in workers’ compensation claim data in the State of California. SCIF is the largest worker compensation insurer in the state, and insures a wide range of employers, including many with operations in construction and agriculture. Reviewing insurance claim data in the state of California for the 2002 policy year, only five back injury claims for agriculture and construction, out of 8,460 submitted, contained the descriptors “stoop” or “squat” in the accident description. Likewise, only two knee injury claims out of 1,687 submitted for agriculture and construction have the descriptors of “stoop” or “squat” listed in the accident description. The low reporting of injuries related to working in stooped and squatting postures in the claim data is attributed to problems with coding the injury information. Claims data are highly dependent on the information shared between the employee, employer, and physician, and also on the understanding and experience of the data entry person. There are multiple opportunities for the specifics of the injury to not be coded into the claims information database.
Current claim forms ask for the following types of information about the nature of the accident:
- Burn; caught in, under, or between; slips, trips, and falls; motor vehicle; strain/sprain; struck by, etc.
- Nature of injury or illness: Specific injury (amputation, fracture, strain, sprain).
- Occupational disease or cumulative injury (cancer, hearing loss, stress).
- Other (angina, multiple, death)
- Body part: Eye(s), neck, shoulder, hand(s), back, knee(s), etc.
There is no place to enter a description of the injured worker's usual work activities. The only activity reported in the claim record is the nature of the specific ‘event’ that caused injury. Low back and knee disorders related to working in stooped and squatting postures are often cumulative trauma injuries, so their cause-effect relationship becomes clouded by the event-based focus of claims reporting. Improvements in data collection would be needed so that exposure to MSD LBD risk factors, such as stooping, could be reported in the claim information. This would assist Safety and Health Services and Loss Control analysis in determining where to focus injury and illness prevention efforts.
Ms. Banks also presented summary cost data for cases of low back and knee injury, which ranged from US$9,243 to $25,291 per case in 2004.
Average Costs of Back/Knee Injuries
| Type of Injury |
Number of Disability Claims With Surgery |
Average Cost |
Average Cost in Today's Dollars |
Number of Claims, (Dis and Non - Dis),With No Surgery |
Average Cost |
Average Cost in Today's Dollars |
| Low Back Disc |
269 |
$163,180 |
$256,998 |
379 |
$16,208 |
$25,291 |
| Low Back Strain/Sprain |
5,152 |
$81,837 |
$138,908 |
111,749 |
$7,131 |
$11,558 |
| All Low Back |
5,750 |
$85,350 |
$144,026 |
118,606 |
$7,176 |
$11,635 |
| Knee Strain/Sprain |
7,874 |
$43,494 |
$74,738 |
27,907 |
$5,592 |
$9,243 |
Information based on data supplied by CWCI's ICIS Database.
Data represents 70% of all California carrier reported claims results, during the period 1996 -2000.
Total claims sample size is: 1,262,401
Data sorts written and analyzed by Jeff Tiedeman - 6/10/04
Courtesy SCIF |
Regulations to control stooped postures in the workplace have, at times, shown a clearer recognition of the problem. In the United States, the state of California enacted legislation in 1975 that prohibits the use of short-handled tools, such as the short-handled hoe, in agricultural operations [CCRs, Title 8, §3456. Hand-Held Tools]. Debilitating back injuries among farm workers were attributed to its use, which required a stooped, squatting, or kneeling posture. Support for this legislation by farm labor advocates and labor unions was based on the hope that long-handled tools used in an upright posture could do the job of weeding, thinning, and hot-capping (manual flaming by torch). However, because the legislation did not prohibit performing these tasks by hand, at ground level, hand weeding became a common replacement for short-handled tool use. After years of debate between growers and farm labor groups, an additional amendment to this legislation was approved in 2004 that closed the hand-weeding ‘loophole’. The new legislation prohibits hand weeding, hand thinning, and hand hot-capping in agricultural operations unless there is no viable alternative. This amendment also provided that if no alternative exists, then every employer engaged in hand weeding, hand thinning, and hand hot-capping is required to add an additional five minutes of rest period time in the middle of each work period. Regulation of the short-handled hoe and its recent expansion to control hand weeding show that stooped work in agriculture is a continuing problem of concern.
Regulations for controlling stooped and squatting postures at work have also been established in European countries that have established a national ergonomics standard. Dr. Lundqvist provided details of the provisions of the Swedish Work Environment Act [
http://www.av.se/inenglish/index.aspx ]. The basic principle of the Swedish Work Environment Act is that a balance between the requirements of the job and human capacity shall be created primarily by adapting the work to the human being, and that ergonomics for the prevention of musculoskeletal disorders is the responsibility of the employer. It specifies that the employer shall as far as is practically possible, design and arrange work and workstations in such a way that the employees can use work postures and working movements that are “…favorable to the body”. The Act recognizes that optimal work level approximates elbow height, and stipulates that prolonged or frequently recurring work with the trunk of the body bent or twisted and with the hands above shoulder height or below knee level shall be avoided. The same applies to work that entails the exertion of force in such unfavorable work postures. By clearly stating that the problem of stooped work is the employer’s responsibility, much more impetus is provided to implement interventions to control it.
What has been learned about the scope of the problem?
As examined in this session, the problem of stooped and squatting postures in the workplace is global in scope and widespread in many industries. However, the full scope of the problem is not well reflected in occupational injury data because current reporting methods do not examine the relatedness of an injury to stooped and squatting work postures. Firmly establishing the risk of working in stooped postures comes only by evaluating the scientific basis for understanding the effects of stooped and squatting postures in the workplace.
In the second session of this conference, researchers from the fields of epidemiology and biomechanics presented their perspectives of the scientific basis for understanding the effects of stooped and squatting postures in the workplace. The researchers examined the evidence that establishes the problem of working in stooped and squatting postures, and they reviewed the risk factors associated with work in stooped and squatting postures and their effects on tissue damage and dysfunction, pain, and injuries. This session’s summary assesses the contributions of the fields of epidemiology and biomechanics to our understanding of the effects of work in stooped and squatting postures and what new discoveries are needed to enhance our understanding.
Leading the conference’s examination of the epidemiology of stooped and squatting postures in the workplace was John Rosecrance of Colorado State University. Using his presentation as a basis, this review proceeds by examining the epidemiological evidence presented in this conference associating working in stooped and squatting postures with MSDs and LBDs.
Epidemiological evidence associating working in stooped and squatting postures with increased MSD and LBD risk
Although Ramazzini wrote of a relationship between the deformities of dockworkers and their stooped work postures in 1713, very few studies
specific to working in the stooped postures are found in the modern epidemiological and biomechanical literature. Some exceptions are:
- Gallagher et al.(1992; 1988; 2002) – confined spaces/ mining
- Estill & Tanaka (1998) - blueberry harvest
- Friedrich et al. (2000) - sewage workers
- Marshall & Burnett (2004) - sheep shearing
In epidemiology studies, stooped work is often categorized as work in
awkward postures, which includes squatting, stooping, non-neutral trunk postures, and lifting. The NIOSH Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders (NIOSH, 1997), which reviewed nine studies on awkward postures and found evidence of an association with LBD, included kneeling, squatting and stooping in the same classification. Thus, more epidemiological evidence regarding the problem of stooped postures in the workplace can be uncovered by reviewing postural studies for references to stooping. Following are several studies of awkward postures providing strong evidence of an association between working in stooped postures and LBDs.
The epidemiological evidence linking working in stooped postures to LBDs is considerable, but only when findings related to stooped work are partitioned out of the more general category of ‘awkward postures’. To focus specifically on the epidemiology of the problem of stooped postures in the workplace requires refinements in future research. First of all, the research community needs to differentiate between stooped posture and stooped work by determining an exposure level at which flexed posture becomes ‘stooped work’ (e.g., work below knees > 40% of time). Secondly, there is a need to develop practical and objective measures of exposure to stooped work (degree of bending, duration, frequency) and to refine the epidemiological case definition of outcome (symptoms, physical findings, diagnoses) for a deeper focus on the effects of stooped work.
Many jobs associated with stooped postures also have high exposure to kneeling and squatting. The studies of awkward posture discussed above also contain evidence linking kneeling and squatting at work to LBDs, although the risk appears more moderate than in stooped postures. Dr. Laura Welch, M.D., Medical Director of the Center to Protect Workers’ Rights, presented evidence associating kneeling and squatting at work with knee disorders. The knee is an inherently unstable joint with potential for movement in four directions. Knee disorders that are caused or aggravated by postural demands of work include osteoarthritis, pre-patellar bursitis, meniscal tear, and cartilage injuries such as chrondromalacia patella. At least sixteen studies, including the NHANES prospective study and the Framingham longitudinal study, show that jobs with knee bending and jobs with heavy work are associated with an increase in osteoarthritis of the knee. A case-control study of meniscal injury (Baker et al., 2003) showed high odds ratios in jobs requiring either squatting or kneeling for more than one hour per day. Bursitis of the knee is associated with jobs requiring kneeling, including coal-mining, where the condition is referred to as “beat knee”, and for carpet layers, especially when using a knee-kicker device. Building trades with prolonged kneeling have a five fold increased incidence of fluid in the knee compared to other construction workers. Clearly, frequent kneeling and squatting postures in the workplace are significant contributors to MSDs of the knee and lower back, and should be avoided as substitutes for stooped work because of the MSD risks of these postures as well. Dr. Welch made the point that workers are often, “Between the proverbial rock and a hard place”. Ergonomics interventions should address the root causes of awkward postures, rather than place workers in the position of having to put one part of the body at risk to relieve pain in another.
- Anderson et al. (1987) - cross-sectional study of males in many occupations: disc disease higher in those required to adopt a chronic stooping posture at the place of work.
- Punnett et al. (1991) - auto workers: significant association between non-neutral work postures, reported strong association of the time spent in non-neutral postures (mild or severe flexion) with back disorders.
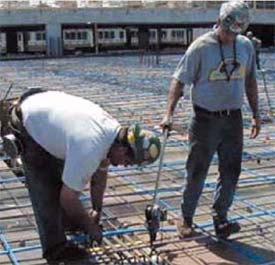
- Burdorf et al. (1991) - concrete workers: significant association of awkward postures with back pain.
- Goldsheyder et al. (2002) - mason tenders: significantly increased prevalence of LBP symptoms with work tasks described as “Bending or twisting back in awkward way”.
- Holmstrom et al. (1992) - construction workers: significant association of LBP with either stooping or kneeling more than four hours per day.
- Marras et al. (1995) - sample of jobs from several industries: back pain multi-factorial, best prediction of high risk jobs from a combination of five variables: load moment, degree of sagittal flexion, lifting rate, lateral velocity, twisting velocity.
- Meyers et al. (2001) - farm workers: review MSD data from three vineyard companies with the majority being back strain injuries. It established priority risk factors for back injury: repetitive lifting of heavy loads, repetitive exertion of force by the trunk and upper extremities, and repetitive or sustained awkward postures of the trunk (including full stoop and twisting with loads).
- Merlino et al. (2003) - construction apprentices: 54% of apprentices indicated the presence of work-related low back symptoms in previous 12 months; 17% saw physician for work-related low back pain in previous 12 months. “Bending and twisting the back awkwardly” and “Working in same position” were both significantly associated with 12-month period prevalence of LB symptoms, and both were judged by workers to be the most problematic job factors contributing to pain and injury.
Biomechanics, the study of the forces on the living body, was discussed by Professor William Marras of The Ohio State University, and Sean Gallagher of NIOSH. When applied to the problem of stooped postures in the work place, it advances our understanding of how the risk factors of working in stooped and squatting postures affect the human body, and how the effects on the body’s tissues lead to the outcomes reported in the epidemiological evidence. Biomechanics allows risk factors and outcomes to be quantified, thereby helping to assess how much of a particular risk factor is too much. Quantification also improves the efficacy of ergonomics interventions because it makes it possible to focus change on the most important risk factors.
Numerous factors have been shown to affect LBD risk; they can be at the physical, individual, or psychosocial level, and are often interrelated and co-contributors. For example, complexity of the task, personality of the individual, and the psychosocial factors of a stressful environment have all been shown to increase loading on the spine.
Most biomechanical studies focus on quantifying physical factors because they are governed by physical laws for which mathematical models exist or can be developed and have the most predictable outcomes when changed. Many biomechanical studies have been conducted to determine the physical factors that contribute to LBD risk. In a comprehensive review of the evidence related to WMSDs, the National Research Council (NRC) and Institute of Medicine (2001) concluded that there is a clear relationship between back disorders and physical load, with the main physical risks factors being manual material handling (MMH), load moment, frequent bending and twisting, heavy physical work, and whole-body vibration. The physical risk factors of MMH, load moment, and frequent bending and twisting are present in work in the awkward postures of stooping, squatting, and kneeling. The effects of working in awkward postures on biomechanical loading and the effects of such loading on tissue outcomes are explored in the following sections.
LBD risk is a function of a person’s ability to withstand a given magnitude, velocity, and frequency of biomechanical loading. An individual’s tolerance for a given loading pattern is mediated by several factors:
- Job Factors
- Working postures
- Duration of exposure to the load and available
recovery time
- Availability of physical support for the trunk
and upper body
- Work environment (e.g., noise level)
- Individual Factors
- Age, Gender, Strength, Endurance, etc.
- Pain Perception
- Genetic Factors
- Psychological Factors
- Psychosocial and Organizational Factors
- Co-worker/supervisory support
- Monotony of work
- Interaction with superiors
Spinal Tissue Biomechanics
Discussing the spinal tissue biomechanical research related to stooped postures in the workplace begins by reviewing the basic principles of spinal biomechanics and seeing what they can teach us about the problem of stooped work. The combination of the spine’s structure and the body’s ability to generate internal forces results in the ability to resist external loads, analogous to a construction crane. Internal forces not only control position and movement of the body but also counteract external loads created by holding an object, resisting impact or vibration, imparting motion to an object, and so forth. There are two types of internal forces: active forces created by muscle contraction, and passive forces created by stretching of tendons, ligaments, and fascia and by compression of joints. Because the moment arms of internal forces are much shorter than those of external loads, the magnitudes of these counteracting internal forces are many times greater than the simple forces of the external loads. As the body moves into a stooped posture, the electromyographic (EMG) activity of back muscles increases and then decreases when full flexion is reached, a point when passive structures (e.g., ligaments) absorb the load. The net effect of both active and passive internal forces is increased compressive and shear forces on the spine’s intervertebral discs, which can lead to herniated or slipped discs and nerve impingements.
A biomechanical injury occurs when the stresses applied to a tissue exceed its structural strength and produce tissue damage, either at the micro or macro level. There are two classes of biomechanical injuries: acute and cumulative. Acute injuries occur when an overload on the tissue exceeds its tolerance. Most occupationally-related injuries are cumulative, developing due to a decreasing tissue load tolerance with repeated loading. The repetition can cause fatigue, and the tissue tolerance decreases below the magnitude of the load. Spinal tissues have the ability to adapt to increased loading and activity. Moderate loading appears protective because it raises tissue tolerances through tissue remodeling. However, excessive loading reduces safety margins, and excessive repetition can decrease tissue tolerance through cumulative trauma.
Low back injuries can take the form of endplate fractures, and/or the disruption of intervertebral discs, muscles, facet joints, or ligaments; such injuries cause the majority of low back pain cases. On the clinical level, it is difficult to identify the cause of a high proportion of low back pain cases. However, researchers have established several pain pathways in the various spinal tissues. These pathways to pain follow a sequence of events consistent with cumulative trauma: accumulated micro-damage decreases tissue tolerances and leads to increases in inflammatory agents, and further loading leads to an increased inflammatory response, greater sensitivity, and finally the perception of pain.
The most common structural damage observed in experimental loading studies of spinal segments is endplate fracture, most often due to fatigue failure. Accumulation of endplate microfractures is a key contributor to disc degeneration, one of the most problematic low back disorders. Endplate failure can result from repeated loading at submaximal levels. The pathway to low back disorders resulting from this type of cumulative trauma injury is well established and was summarized at this Conference as the following:
Sequence of Events in a Low Back Cumulative Trauma Disorder
- Phase I: Endplate Fractures
- Spine loaded in some combination of compression/shear
- Resulting Disc compressed
- Loss of fluid
- Reduction in space between vertebral segments
- Loss in ability to withstand further compression/shear forces
- Endplate micro fractures
- Endplate heals via scar tissue
- Scar tissue inhibits flow of nutrition to disc
- Phase II: Disc Degeneration
- Decreased disc nutrition leads to fissures in the annulus fibrosis
- Disc nucleus migrates via fissures
- Inflammatory nucleus material contacts pain fibers in periphery of disc
- Low back pain results
- Decreased tolerance and work capacity
Working in Awkward Postures
This section builds an understanding of the effects of work in awkward postures on biomechanical loading. The effects of work posture on biomechanical loading and on energy expenditure are explored for manual materials handling (MMH) and for static postures at low working heights and in vertically-restricted workspaces.
Intervertebral disc pressure is affected by external loading, and increasing as the result of increasing external load in the hands, increasing trunk flexion, or a combination of both. When lifting in trunk flexion, spinal loads may be 2-3 times that in the neutral posture. In addition, load bearing in the spine changes due to flexion. In the neutral posture, approximately 20% of the compressive load is carried by the facet joints and the other 80% by the disc; in the flexed posture, 100% of the compressive load is carried by disc. At higher degrees of flexion, such as during stooped work near ground level, peak stresses increase due to stress concentrations on the anterior portion of the disc. When working in a stooped posture, even light loads in the hands can produce high internal forces and disc pressures.
Most studies of lumbar motion segment load tolerance have concentrated on ultimate strength in compression. Only a handful has examined fatigue life, and none has simulated the spinal loads that result when lifting a load in different torso flexion postures. This creates a great gap in our understanding of the way in which the increased loading on the spine due to lifting in the flexed posture affects the fatigue life of the spinal tissues.
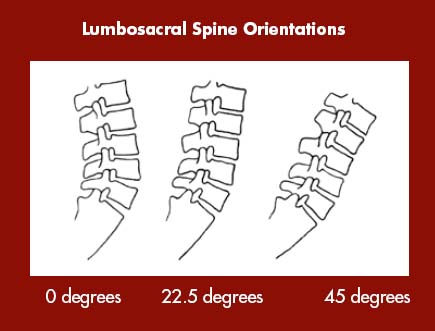
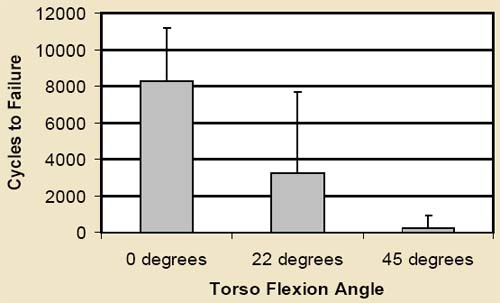
The main objective of the Gallagher-Marras study (Gallagher, 2002) was to quantify the fatigue life of lumbar motion segments when loaded to simulate lifting a 9-kg load in the hands at three torso flexion angles (0, 22.5, 45 deg.). The results of the study indicate that torso flexion angle had a highly significant effect on the tolerance of the spine to fatigue and biomechanical failure. Lifting in full flexion had a tremendous impact on fatigue failure, with fatigue life forty times less at 45 degrees of flexion from neutral. These results suggest that the rate of damage in full flexion likely exceeds the body’s ability to remodel damaged tissue, but remodeling may be possible in other postures. The findings of this study provide important implications for stooped postures and for lifting recommendations. Many of the current tools for assessing the LBD risk from lifting suggest a modest decrease in weight for loads lifted in flexion. The discounting factors for frequency of lifting are often independent of torso flexion angle. The results of this study suggest that both the weight of loads and frequency of lifting should be dramatically curtailed when the spine is in flexion, with important implications for job design. The results indicate the critical importance of designing workplaces to avoid lifting in full flexion. Further research into LBD risk assessment for other stooped activities, such as pulling cables or pushing loads in a flexed position, is recommended.
Spinal Failure And Flexion (Gallagher, 2002)
Sean Gallagher of NIOSH also presented research on the effects of MMH in stooped, squatting and kneeling postures in vertically-restricted spaces on spinal load and on worker performance. Such postures predominate in workspaces such as low-seam coal mines, airplane cargo holds, and utility tunnels. Research on lifting in kneeling yielded decreased lifting ability compared to stooped and standing postures. Psychophysical studies have shown that there is a 10-20% reduction in lifting capacity when kneeling as compared to either stooping or standing erect, which were comparable to one another. A study of trunk extension strength when kneeling showed a decrease of 18% compared to standing, due to the loss of lower leg assistance when lifting in the kneeling posture. Moderate vertical space restrictions cause workers to stoop or squat, which increases the torque on the spine compared to standing. Further vertical restriction forces workers into a kneeling posture, which also produces much higher spine loads than standing. The results of these studies indicate that all three awkward postures (stooped, squatting, and kneeling) increase the load on the spine.
|
|
Baggage handling in an airplane cargo hold, with lumbar motion monitor (right)
|
Several researchers have examined energy expenditure in awkward postures. Findings indicate that the choice of posture by the worker is often determined by the energy demands of the operation. A stooped posture is most frequently used for high energy consumption activities, and either standing, squatting, or kneeling (depending on the height of the operation) is used for low energy-demand tasks. Stooping is favored for high energy tasks because the upper torso is supported by the passive tissues of the back (e.g.,spinal ligaments), reducing the energy demands and making more energy available for work. Kneeling and crawling have high energy costs and a much slower speed of movement, so it is observed in tasks requiring lower energy expenditure, and where the worker does not have to move as much. Because stooping is favored for high-energy consumption tasks, the LBD risk in these tasks tends to be higher because the risk of working in a stooped posture is often combined with that of forceful exertions.
Stooped posture is found to affect the ligaments and spinal muscles, increasing the spine’s risk of injury. Animal studies indicate that laxity in spinal ligaments and other passive tissues increases after periods of either repeated flexion or static flexion (Olson et al., 2004; Solomonow et al., 2003). In a laboratory study with 18 human subjects, Granata et al. found that work activities requiring static lumbar flexion for 15 minute periods contributed to changes in the reflex behavior of the paraspinal muscles (Granata et al., 2005). Both laxity in the passive tissues and the observed changes in reflex behavior of the paraspinal muscles may decreases spinal stability, leaving the spine more vulnerable to injury.
Although the epidemiology identifies working in a stooped posture as being associated with increased LBD risk, some ergonomics analysis techniques fail to identify the elevated risk of stooping (Snook, 1985). Psychophysical methods, which measure the willingness of subjects to exert themselves during the test, yield lifting capacities that are comparable in stooping and standing. Energy expenditure and back muscle activity is often lower in stooping than other postures, since the weight of the trunk is supported by ‘hanging’ on passive tissues (ligaments). Trunk extension strength in the stooping posture is much higher than in kneeling, largely due to the ability to use the large and powerful hip extensor muscles more effectively. However, neither trunk extension strength nor energy expenditure is a good predictor of the risk of low back injury in a flexed posture. Relatively high lifting capacity, lower energy costs and muscle output, and increased mobility compared to kneeling may be perceived by workers to be advantages of stooping, and help explain why the stooped posture is the most common awkward posture in the workplace, despite its association with LBD.
Conclusions about the scientific basis of the problem
Clearly stooping, squatting, and kneeling all have major risks that are evident from studies in epidemiology and biomechanics. If stooping is frequent, fatigue failure in the spine can occur more rapidly because the recovery of damaged tissue may not be adequate to withstand subsequent forces. Repeated or sustained stooped postures may also disturb the neuromuscular and ligamentous stability of the lower back, leaving the back more vulnerable to injury.
Kneeling and squatting are often seen as alternatives to stooping as a way to work at low levels without bending the back as much. However, these postures are also significant contributors to MSDs of the knee and low back, with high odds ratios in jobs requiring either squatting or kneeling for more than one hour per day. Job improvement efforts should target reduction of existing risk factors, while avoiding increased risk to other regions of the body.
To improve our understanding of the biomechanics of the spine and the lower extremities in the stooped posture, there is a need for research studies designed to evaluate the effects of these postures on tissue responses under various conditions and loading patterns. Research is required to understand how the intervertebral disc, the meniscus of the knee, and other passive tissues respond to repetitive versus static loading. Epidemiology and biomechanics provide much of the basis for understanding the effects of working in stooped and squatting postures, and the knowledge gained from such study should be incorporated into the case definition of stooped work, and in job design criteria that take into account the tissue fatigue generated by static postures.
Reducing the exposure to stooped and squatting postures in the workplace is a challenge for employers, employees, and for the occupational safety and health community. In some workplaces, ergonomics interventions may obviate the need for workers to stoop or squat. In other cases, it may not be possible to eliminate these work postures. For example, in agriculture and construction, the location of the work is often at or below knee level, and in mining or utility work, the work environment may have a vertical height restriction. The fact that these physical workplace conditions are difficult to modify has often led employers and/or employees to feel that nothing can be done to address the problem. However, at least some control of the risk factors associated with stooped and squatting postures in the workplace is usually possible. The second day of this conference was devoted entirely to presentations and discussions on ergonomic intervention strategies and technologies for mitigating stooped and squatting postures in the workplace.
- Talk to management and employees about their concerns and the reasons for concern
- Look for variables that help characterize the current risk (injuries, medical visits, productivity, absenteeism, turnover, quality or performance problems)
- List the activities / tasks performed in the jobs of interest
- Choose the activities of most concern to the workers
- Observe the activities and quantify the risk factors
- Identify the interactions between risk factors (e.g., stooping and exerting high force)
- Prioritize which risk factors should be addressed
- Facilitate problem solving with workers - the experts on the job
- Identify why the risk factors are present
- Develop strategies to reduce the risk
- Identify strategies most likely to succeed
- Implement solution(s) after communications and feedback on pilot study
- Assess: do a follow-up evaluation of the job/task using same measures as earlier
- Importance of using their numbers whenever possible – ask them for data
- Importance of addressing a problem they perceive as a problem
- Show them a videotape of their operation after it was analyzed
- Involve them in problem-solving after using the videotape to define the risk
- Identify root causes that they have control over
- Conservatively project the expected benefit of a consensus solution
- Identify the probable costs/ impact of doing nothing about the risk factors
- Have them set up an action plan for implementing and evaluating the change
- Be a facilitator, not the ‘doer’
Controlling stooped and squatting postures in the workplace begins by having a strategy in place to identify risk factors, determine their root causes, and develop and implement ergonomic interventions. Considerations for evaluating workplace interventions were presented by ergonomics consultant Suzanne Rodgers. Static postures, such as stooping, may not be obvious as problems to workers or management, so there is a need for a well-defined strategy to
quantify the risk of stooped work and market the benefits of change to all concerned. It starts by persuading management that there is a problem, through assessing the entire workplace environment, not just the physical load, and including labor and management in identifying the problem, identifying root causes that they have control over, and setting up an action plan for implementing and evaluating change. Data about the job should be assembled so that a clear case for change can be made, including a cost-benefit analysis to document the potential benefits of an intervention. For example, the toughest jobs may be hard to fill, with high turnover. A job with long periods of stooping or squatting may produce a ‘natural selection phenomenon’ so that only a small number of workers can ‘survive’ in the job for more than a short period of time. This is a ‘flag’ indicating a problem, and associated costs to hire and train new workers to fill the vacancies left by those who have moved on.
Selling change to the workers requires having them involved throughout the process, from beginning to end, for their valuable knowledge about the jobs they perform. To enhance worker acceptance, implementing a change should begin with their involvement in problem solving new approaches to the task: developing different procedures, choosing new tools, building a mockup, and then designing a pilot project with reduced production pressures during a trial period, so that workers can practice and critique it before introducing a major change on the job. Unless there is a serious safety issue, give the workers the opportunity of accepting, modifying, or rejecting a strategy. It is important to involve all shifts and related workers (e.g., tool/ equipment maintenance) in the process. If a new tool or piece of equipment is added to the job, provide training about its use and time for workers to learn to use it comfortably. We should recognize that strong external pacing and production standards, including incentive systems, make it difficult for workers to find their best work pace and can result in fatigue and overexertion injuries.
Ergonomics evaluations should, where possible, include a cost-benefit analysis to show the advantage of a making a change. The effectiveness of ergonomic interventions can be measured in several ways. Direct methods include:
- direct and indirect workers’ compensation costs for people working on the job
- frequency of accidents/incidents
- lost time days
- restricted time days
- training time on the job; cost of replacement workers
- productivity, including effects on the time of supervisors and others handling claims
- quality/performance
Other indirect costs should also be factored into the cost-benefit analysis. These include absenteeism associated with the job, turnover on the job, and the costs of temporary and replacement staffing. This holistic view of the benefits of ergonomics interventions should provide even more motivation for implementing change.
A key element in a successful strategy for workplace ergonomics is a participatory action team. This involves the establishment of a multi-disciplinary ergonomics team that includes labor, management, engineering, and other members who can provide valuable input in the process. The ergonomics team performs four main tasks:
- Ergonomics evaluation of job tasks
- Assessment of production problems, worker symptoms and injuries, and associated costs
- Evaluation of alternative interventions
- Recommendations to managers
Ergonomics teams of this type in many large corporations have shown tremendous success in addressing ergonomic problems. It is important that they receive appropriate ergonomics training, applicable to their industry, in order to proceed in an efficient and effective manner.
The hierarchy of controls by which change may be accomplished includes: 1) engineering controls – to eliminate exposure or eliminate the high-risk task altogether; 2) administrative controls – to reduce exposure; and, 3) behavioral controls – to improve work practices. This is not a simple hierarchy by which one control is selected over the other. Rather this is a set of opportunities from which an optimal combination of interventions should be developed.
Determining which controls are available as interventions to the problem of stooped work is challenging for the industries of concern, especially agriculture and construction, because they have tremendous variation in their workplace environments. Addressing the challenges within these industries necessitates focus on each of them individually. The remainder of the Conference concentrated on understanding the reasons why stooped work is so common in agriculture and construction and what interventions are available to address these root causes of the problem.
|
|
Rolling table for transplanting |
Handles as ‘arm extensions’ |
| |
|
|
|
Lifting pots by hand |
Using nursery handles |
To address the problems of stooped and squatting postures in agriculture, realistic and effective interventions must be developed and implemented. Management-union ergonomics teams have proved successful in manufacturing; such a team for agriculture should include:
- Farm workers
- Farmers
- Farm organizations
- Agricultural industry specialists
- Ergonomics specialists and other people with nonagricultural backgrounds
- The ‘younger generation’
At the top of this list are the farm workers themselves. Looking back at the history of technological innovation in agriculture, most major breakthroughs were initiated by farmers driven to improve their workplace. There is a need to increase worker participation in developing ergonomic interventions for stooped and squatting work, in order to provide the feedback on efficiency, comfort, and social and cultural issues that is necessary to improve worker acceptance and understand barriers to adoption. As an example of the importance of ethnocultural issues, prone workstations were rejected by East Indian workers in one California operation because it is not acceptable in their culture for women to be lying down in the company of men. Such ethnocultural barriers may be broken down only through a participatory approach to ergonomics.
Engineering Controls for Agriculture
John Miles, of the Agricultural Ergonomics Research Center (AERC), University of California at Davis, presented a classification of the engineering controls for stooped and squatting work in agriculture. The three classes of interventions are: 1) Reduce or Eliminate the Need to Stoop or Squat; 2) Mechanical Worker Protection or Worker Aids; and, 3) Fully Mechanized Operations. These classifications provide a useful framework for discussing the intervention strategies presented by other researchers.
1. Interventions that reduce or eliminate the need for stooping
Reducing or eliminating the need for work in stooped postures can be accomplished by changing the physical work space or by giving the workers tools that allow them to interact with the workplace differently. There are several changes that can be made to the spatial workplace in agriculture. One is to raise the beds in which crops are grown, such as for strawberries. It should be noted that even though strawberry beds are raised — LBD risk is lowered — the fact remains that the amount of stoop is still very high. However, raised beds and the related improvements are not feasible for all crops, such as cilantro and other leafy greens.
Nursery and greenhouse settings offer a higher level of control over the geometry of the workspace, where it is more feasible to grow crops on raised beds or on tables. One adaptation for greenhouses is the use of revolving carousel tables to increase the growing area while offering an adjustable working height. An alternative to changing the geometry of the growing environment is to change the geometry of the crop itself. This could consist of growing taller plants: breeding or bioengineering plant varieties with the harvested commodity located at a more comfortable height for the worker.
Employers can provide portable tables or carts, and lifting aids, so that work operations can be performed at better working heights. The UC AERC team was successful in developing adjustable handles for use in lifting and carrying potted plants that significantly reduce the need to stoop or squat. These handles led to major reductions in spinal flexion, hand grip force, and in Lifting Index calculated using the NIOSH Lifting Equation, without compromising productivity or energy expenditure (Janowitz et al., 1998; Meyers et al., 1997).
Improved hand tool design may also reduce or eliminate the needs for stooped or squatting work. Dr. Kumar and the IARI team have been successful in optimizing tools to reduce the risk of stooped posture work. An example is an improvement for rice paddy plowing. This job has high energy consumption and necessitates the use of a stooped posture to regulate forces applied to control plow depth. The research team determined an optimal height for the plow handle by studying user comfort, applied force, and oxygen uptake for different plow designs.
These examples illustrate that simple low-cost solutions can be developed for controlling the problem of stooped postures in agricultural work, but are often only realized through the combined efforts of an ergonomics team.
|
|
UC AERC Human-powered prone cart |
UC AERC Motor-driven prone cart |
2. Mechanical Worker Protection or Worker Aids
Mechanical worker protections or worker aids act to reduce the physical loading on the spine by reducing or eliminating the stoop or supporting some of the load during a stooped or squatting posture. There are three types of mechanical worker protections and worker aids that were discussed as having the potential to control stooped postures in agricultural production work: devices for kneeling, prone workstations, and load transfer devices.
Improving kneeling comfort
Kneeling postures dominate in work that is very low to the ground and demands a high level of hand-eye coordination. In agriculture, such kneeling work is common in plant propagation for nursery and ornamental plant production. To reduce the discomfort of kneeling, workers can use knee pads. Even with knee pads, however, kneeling and moving around on a rough soil surface can still be very uncomfortable. A much more stable kneeling surface can be provided by padded knee boards. They consist of a board covered with upholstered foam padding that offers protection for the shin and feet in addition to the knee. All-terrain wheels allow the boards to roll forward and backward through the field. Because pushing while kneeling is difficult, the UC AERC has developed a knee board with a hand-powered ratchet to drive the wheels. This knee board also has a storage area for frequently accessed tools and materials so workers do not have to twist or bend as much. Though it is questionable how much knee pads or knee boards prevent the WMSD risks of working in a kneeling posture, favorable worker acceptance indicates they reduce some of the strain from the work.
Prone workstations
The stooped posture can be eliminated in many agricultural tasks, such as harvesting or weeding, by using a workstation that supports the body in a more neutral spinal posture, such as lying prone or sitting upright. Most development has focused on prone posture workstations because workers rarely have to deviate from a neutral spinal posture; in sitting posture workstations, the worker still has to frequently bend or twist the back to reach the plant material. Several researchers at this conference discussed the potential of prone workstations for controlling stooped postures in agricultural work. Robert Meyer, a graduate student at the University of Wisconsin, presented his research on the development of prone posture workstations for agriculture as well as studies comparing the biomechanics of work in stooped postures versus prone postures.
Prone work platforms can take the form of human powered individual carts, self-propelled individual carts, or platforms with multiple prone workstations attached to a tractor or with their own integrated power unit. Most of the current development is occurring in Europe, although interest is increasing in North America. Prone picking devices first appeared on American farms about 50 years ago. Early development focused on mechanical design and improving productivity, while comfort seemed secondary. American Society of Agricultural and Biological Engineering papers from the 1970’s describe their use in strawberry and nursery operations and report productivity increases and acceptance by workers. Subsequent development has centered on making prone workstations more comfortable. Researchers from the UC AERC have built and tested several human-powered and self-propelled carts. The University of Wisconsin has developed guidelines for human-powered seated and prone cars, and tested some of the currently manufactured self propelled models.
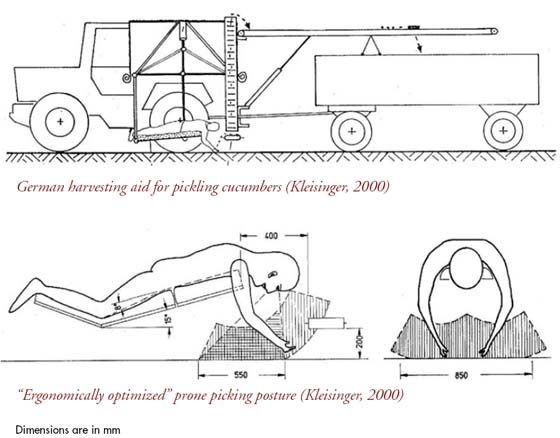
There are currently no commercial manufacturers of prone workstations in the United States. Almost all of the commercially available self-propelled prone workstations are designed and manufactured in Europe. There are at least two German manufacturers of motorized prone workstations (d‘Heureuse Inc.; Kress Inc.), and another German company has produced a tractor-mounted, multi-station prone work platform used in cucumber harvesting. The Swedish Drängen is a single-person, track driven motorized machine with a very adjustable and well-padded workstation. The Ryömijä is a battery-powered, wheeled single-person machine produced in Finland with an adjustable workstation similar to the Drängen’s. Unfortunately, the European models are relatively expensive and are either not exported to the U.S. or, in case of the Drängen, lack local technical support. Given the relatively simple level of technology involved, it is entirely possible that similar designs could be manufactured in the U.S. should prone workstations gain popularity.
There are several issues to consider in optimizing the prone workstation for comfortable and efficient work. The first issue to consider is the prone posture itself: whether the body should be completely straight and horizontal or whether the arms and legs should be bent with the trunk inclined or declined. Underwater and zero gravity studies have identified a ‘neutral’ body posture with the arms and legs bent at moderate angles, and this has led many to believe that this is the optimal prone posture. The direction of travel (headfirst or feet first) and the need for a head rest is a concern, as these will determine head and neck position.
The pace of work is influenced by whether the prone work platform is a single-person, worker-paced device or a tractor-mounted multi-station unit in which work is machine-paced by the speed of travel for the group. These issues have been the subject of much of the recent research on prone workstations, as more attention has been brought to the problems of WMSDs in agriculture.
Four recent studies, three in Europe and one in the United States, have investigated the use of prone workstations in agriculture from the perspective of worker comfort. German studies by Kleisinger and Rullmann examined different postures, direction of travel and upper torso support in prone workstations for agriculture using motion analysis and EMG activity. The results indicated the lowest muscle activity was with an improved narrower upper torso support, sloped at about 10 degrees, with slightly flexed hips and knees (Kleisinger, 2000; Rullmann, 2003). Because head movement might make it difficult to design a support, and no EMG activity was seen in neck muscles, it was concluded that a head rest is not necessary. In a Finnish study by Mattila et al., productivity and exertion levels were monitored while harvesting low-growing crops using six different methods, of which two were prone carts (Mattila, 2001). The greatest distance traveled was in the traditional stooped posture, but the greatest amount harvested was in the human-powered prone cart. The lowest perceived exertion occurred in both prone cart models, as did the greatest reduction in heart rate compared to the traditional stooping method. In the Netherlands, a 2004 study by Roelofs compared discomfort in four positions (straight prone, bent prone, seated, and stooping) while weeding (Meyer, 2004). Subjects reported lower subjective discomfort with both prone postures as compared with seated and stooping. Recommendations developed from this study included suggestions for improved coverings for the supporting surfaces, using a self-propelled platform because it might decrease whole body vibration (compared to tractor-mounted platforms), and for more research into alternate postures for agricultural work.
In the United States, a NIOSH-funded pilot research project was recently completed at the University of Wisconsin that compared working in a stooped versus a prone posture in a simulated picking and planting operation. Subjects worked for two 15-minute work periods for each posture and rated their discomfort, while EMG and heart rate were monitored. The discomfort ratings were higher in stooped posture, with the greatest differences reported in the hamstring, knee, and low back areas. In addition, heart rates were higher in stooped work than in prone work, and significant differences in muscular activity of the trapezius and erector spinae were detected. The findings of these four studies indicate that prone postures produce lower physical exertion and discomfort than stooped postures; that prone posture workstations are capable of productivity rates similar to or better than stooping or kneeling; and that improvements to prone workstations can be made by using a position with an inclined torso (shoulders higher than hips) with slightly bent hips and knees, and by reducing vibration.
Although the use of prone workstations as an intervention for stooped work shows much potential, several issues need additional consideration. First, more research into human performance issues related to strength, endurance, respiration and circulation, head/neck support, arm support and freedom of movement, and vision, are needed in order to optimize worker efficiency and reduce the risks of prolonged static postures. Areas recommended for further study include improving motorized machines by reducing whole body vibration, improving head support, providing a user-friendly system for workers to set the optimal pace, attention to job rotation and worker scheduling, and developing guidelines for prone workstations that optimize worker comfort and efficiency. Finally, it is necessary to study the economic impact of adoption of prone workstations on both management and workers.
Load Transfer Devices:
Load transfer devices attempt to reduce the load on the lumbar spine by transferring a portion of the trunk weight and external load to the hips and lower limbs. Fadi Fathallah, of the University of California at Davis, presented the results of two investigations that his group conducted on load transfer devices for use in stooped work in agriculture and construction. The first was a laboratory evaluation that assessed four load transfer devices for their ability to reduce back muscle activity. At the time of the study in 2000, three were commercially available; each using a different mechanism to support the upper body while working in a stooped posture (Barrett and Fathallah, 2000). The Happyback, manufactured by Ergo-Ag of Aptos, CA, utilized fiberglass rods and fabric to support a chest harness and transfer torso loads through a pad near the low back to thigh straps buckled above the knees. Bending Non-Demand Return (BNDR) has metal frame segments for the anterior torso and upper legs that are padded at the chest and thighs and connect to a resistive articulation and support belt at the hips. The Bendezy is an Australian design consisting of an aluminum frame with soft shoulder straps around the upper torso, low back pad, and abdominal straps to hold it in place. Resistance to torso load is provided by springs extending from a posterior counterweight lever to straps on the knees and feet. An additional fourth version was tested that consisted of a modified Bendezy prototype with the springs and lower limb straps removed and a posterior counterweight added. The experiment consisted of nine subjects assuming stooped postures and lifting three weights (0, 10, 20 lb) while wearing a device. Each participant rotated through all the devices and performed a stooped lift as a control condition. EMG results showed reduced back erector muscle activity provided by all four load transfer devices. The devices all act to reduce the loading on the back, though the impact of this load reduction on LBD risk is uncertain. Additional feedback from agricultural workers suggested that the concept of load transfer is worth exploring, but that much improvement in comfort, usability, and adjustability would be needed for these devices to be practical.
The second study on load transfer devices concerned the GRIPSystem. It is a set of straps and belts used for two person team lifting and carrying of bulky or heavy objects and functions by transferring loads from the hands to the shoulders and hips, thereby reducing the forward bending moment on the low back (Paskeiweicz and Fathallah, 2006). The laboratory evaluation consisted of subjects lifting three different heavy household items using two approaches: lifting the load in their hands, and using the GRIPSystem. Back muscle EMG and spinal kinematics measured by the Lumbar Motion Monitor (LMM) were recorded for each lift. The results of the trials indicated that lifting using the GRIPSystem resulted in lower erector spinae muscle EMG activity, reduced sagittal flexion, and reduced LBD risk compared to lifting the load using the hands. In addition to reducing the load on the spine, the GRIPSystem would also have the effect of reducing forward-bent postures often seen when carrying bulky objects, especially up or down stairs. The concept employed by the GRIPSystem, which does not depend on a wheeled device for transporting the load, should be explored for use in agriculture and construction tasks.
Personal load transfer devices show the potential of providing significant reduction in loads imposed on the spine during stooped work. Further research is needed to evaluate their efficacy in reducing LBD risk, as well as possible discomfort in other body areas, such as the legs. More attention to anthropometric and comfort issues is needed in order to increase the feasibility and usability of such devices. It is hoped that successful devices will become available to reduce the LBD risk of stooped work when other means of modifying the workplace are not possible.
3. Mechanized Operations
Mechanization of agricultural tasks has the potential to eliminate the need for stooped and squatting work. Past successes include the cotton picker, hay mower, mechanical planter, and the processing tomato harvester. Though these inventions have the desirable benefit of reducing stooped work, their successful implementation occurred primarily because they tremendously increased productivity. History shows that while each technological advance reduced or eliminated one form of manual work, with it came new ergonomics problems. Movement to mechanization may eliminate stooped work, but may increase exposure to other risk factors for equipment operators such as noise and vibration, static work postures, and repetitive motion. This is an important consideration in developing engineering controls for stooped and squatting postures in the workplace.
Despite the success of mechanization in many areas of agriculture, the production of most fruits and vegetables, even in industrialized nations, continues to be highly reliant on hand labor to perform many essential work tasks, especially harvesting and weeding. Currently, fully mechanical harvesting methods are not yet technically and/ or economically viable in many fruit and vegetable crops, especially for those intended for the fresh market, because they create excessive mechanical damage and cannot be used in crops with indeterminate maturity.
Despite these limitations, several vegetable and fruit crops can currently be harvested mechanically; the UC Davis Postharvest Technology Group website (http://postharvest. ucdavis.edu) provides links to several manufacturers of fruit and vegetable harvesting equipment. For fresh market produce, possibilities exist to develop machines that redefine the ergonomics of the working environment. The stooping that is necessary to cut vegetables at ground level for harvest can be eliminated by using a machine that cuts them and elevates them to waist height for sorting and packaging. Research work on elevating harvester machines has been conducted at UC Davis for cilantro, and there are models for many leafy vegetable crops, such as spinach and lettuce varieties, that are commercially available in North America and Europe. The use of such machines is increasing annually because of improved productivity and worker approval. Elevating harvesters are showing much promise in reducing the risk from stooped work in leafy vegetable harvest, and their development should be further explored.
|
|
Ortomec leafy vegetable harvester
Photo courtesy of Sutton Agricultural Enterprises, Inc., Salinas, CA |
Spinach hand harvest
Photo courtesy of Sutton Agricultural Enterprises, Inc., Salinas, CA |
Complete automation of agricultural tasks is an emerging technology that can eliminate the need for workers in high risk tasks, especially those requiring heavy lifting and work in stooped postures. The first wide-scale use of automation to replace a traditionally manual labor task was found in automated (robotic) milking systems. First developed in Europe, they have become very common there and their use is expanding in North America, particularly among smaller producers. The automated milking machines save time, eliminate a source of physical strain, and are cost-effective despite their high initial investment costs. Similar breakthroughs in automated agricultural systems are expected in the next 10-20 years, due to promising research currently being undertaken. The problem of stooped work while weeding may be tremendously reduced through a robotic weed control system that uses technologies being developed at the University of California at Davis. Automated selective harvest of tree fruit and citrus is being researched in several industrial nations, and such technology could lead to automated harvesters for fruit and vegetable crops. The outlook for the future suggests increased mechanization in agriculture, and with it, a reduction in the demand for work tasks performed in stooped postures. However, these achievements are still several decades away and do not address the problem in nonindustrialized nations that cannot afford such technology.
Administrative Controls for Agriculture
Engineering controls are preferred for ergonomic interventions, but they are not always practical due to cost, complexity, or usability. In these situations, risk can be mitigated by the use of administrative controls, which use workplace policies, and practices to change the way the worker is exposed to risk. For much of the agricultural work in stooped and squatting postures, no feasible engineering controls are currently available, so reducing the MSD and LBD risk must be accomplished using administrative controls.
There are several administrative controls available for stooped and squatting work in agriculture. Pay structures can be examined to determine if switching from a piece-rate to an hourly wage system may reduce overexertion. Introducing programmed breaks, reducing the number of working hours, or hiring more workers during peak periods may be effective in reducing the demands on the individual worker. Job rotation and work enlargement (more variety in the job with less specialization of tasks), if carefully planned, may be effective in reducing the risk of strain on any one area of the body. Finally, training managers and workers on reducing risks may be beneficial, if this leads to improved work practices and reduced exposures to risk factors for MSDs.
Julia Faucett of the University of California at San Francisco presented her findings of research on rest and recovery breaks as interventions for MSDs (Faucett et al., 2006). The motivation for testing organized rest breaks came from symptom survey results for agricultural workers who frequently kneel or stoop, and who indicated that the low back and knees were the most frequently affected body parts. Previous studies by other researchers who evaluated rest breaks as an intervention for MSDs in computer use, meat and poultry processing, and construction have led to the following guidelines:
Guidelines for Work and Rest Break Scheduling - (Konz, 1998)
1: Minimize the fatigue dose.
2: Use frequent short breaks.
3: Maximize the recovery rate.
4: Use work breaks.
5: Increase recovery/work ratio.
6: Have a work scheduling policy.
7: Optimize stimulation at work.
Current rest break scheduling for agricultural workers does not have the frequency of rest breaks suggested by these guidelines. In California, regulations require that employers allow employees to have a ten minute rest break for every four hours worked and a thirty minute meal period for any worker who works more than 5 hours a day. Dr. Faucett and the UC AERC group conducted a controlled, randomized experiment to assess organized rest breaks as interventions for agriculture (Faucett et al., in press). Two jobs were analyzed: tree budding and grafting in a large tree nursery (primarily squatting and kneeling), and harvesting strawberries (primarily stooping and squatting). Outcome measures were worker symptoms and productivity. Two rest break conditions were tested - the control case having the usual scheduled breaks of ten minutes mid-morning and mid-afternoon and a thirty minute lunch, and the intervention case having additional five minute breaks each hour in which there was not already a scheduled break (approximately twenty additional minutes of rest per shift). The results of the study show that intermittent brief rest breaks appear to reduce the symptoms of fatigue and musculoskeletal discomfort, while productivity appears to be minimally affected. After cessation of the study, workers and managers in the tree nursery cooperatively agreed to continue the use of breaks whether paid on an hourly or piece rate basis. The UC AERC group has seen similar adoption with its engineering solutions for the wine grape and nursery industries (Meyers et al., 2006; Janowitz et al., 1998). Workers continuing to use the intervention are often the best indicators of success.
The findings of this study emphasize the potential of rest breaks as an intervention for MSDs in the workplace, though much more research is needed. One such need is to develop and test optimal rest and work patterns for specific work tasks, such as those requiring prolonged stooping and/or kneeling with and without lifting. Another is to understand the effects of rest break scheduling on MSD symptoms and on other outcome measures such as leg swelling, general fatigue, and heat stress. Lastly, there should be more research to evaluate the effects of rest breaks on health outcomes and on productivity over the course of a work day.
Why Workers Stoop in Construction
- Design features/specifications may dictate heights/sizes/locations of installations
- Intervention: Need for building designers and construction planners to have better understanding and awareness of how the work will be performed.
- Sequencing of construction activities limits space/access to point of installation
- Intervention: Need for construction planners to have better understanding and awareness of how the work will be performed in each stage of construction activity and incorporate this into project scheduling decisions
- Location of the work itself (often trade specific)
- Example: Rebar tying by iron workers
- Intervention: extended handle rebar tying tools and waist-height rebar storage devices
- Example: Flooring installation, painting low areas of walls
- Intervention: knee pads, mats, wheeled support carts (e.g., RACATAC, automotive creeper)
- Example: Stooping to fasten roofs panels or caulk seams
- Interventions:
- auto-fed screw gun extensions
- extended handle caulk/glue guns
- EZ Reacher for site clean-up
- Inadequate tools for the job
- Intervention: Select the proper tool for the job
- Example: drills optimized for concrete floors
- Poorly designed equipment for material/tool handling
- Intervention: upright shelf storage better than standard chest drawer
- Poorly designed work staging/layout
- Intervention: Mitigate low-height work in field design of work layout
- Intervention: store and handle materials properly
- Examples:
- pre-placing materials for upright work in bins or on racks at waist height, rather than on ground
- using two-person lift for heavy objects
- walk-up long heavy items, such as boards
- Combinations of the above
|
In addition to these common administrative controls, several alternative ways of handling the problem of stooped work in agriculture deserve consideration. Growers can promote the concept of a “You-Pick” farm, where customers harvest their own fruits and vegetables for discounted prices. In France, this model has expanded to “tourist farming”, where urban customers get the added benefit of experiencing the activities of rural life. Marketing the qualities of rural living and the traditions of farming may allow manually harvested commodities to be perceived as higher-value, with the extra income being available to pay for workplace improvements. Promoting the benefits of rural life may also be used to improve the psychosocial environment for workers.
|
|
| Photo courtesy: U.S. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. |
Photo courtesy: Construction Safety Association of Ontario. |
Manual rebar tying (left) vs. Use of an extended-handle rebar tying tool (right) |
Controlling for stooped and squatting postures in construction jobs begins with understanding the variation in the workplace, which often changes hour by hour and from one day to the next, from one area of the site to another, and from project to project. The varying workplace and work tasks lead to varying postures, with the postures seen among construction workers often dictated by the pace and the location of the work. The flexibility in the type and location of the work required in construction necessitates a similar flexibility in type and application of ergonomic interventions. The possible combinations of work tasks and work environments in construction are practically limitless. Developing an intervention for each work task is impractical. An effective approach for controlling stooped and squatting postures in construction is determining the reasons for work in these postures and then proceeding to develop interventions that mitigate the causes of the problem of stooped and squatting postures, rather than addressing the problem on a task-by-task basis. This approach was presented by Billy Gibbons, President of the consulting group DGI Ergonomics & Safety Leadership Inc., who presented several causes of the problem of stooped and squatting postures in construction work and interventions designed to address them. Following is a listing of the common reasons why workers stoop or bend in construction and some examples of the problems and possible interventions to mitigate their causes.
Often, construction workers have the skills and tools necessary to develop and fabricate interventions quickly. Yet they often say that time constraints and the need to move on to a completely different set of tasks are the reasons for not attempting to mitigate ergonomics problems. In the construction industry there is a need for short-term “quick fixes” that can be applied to a wide variety of tasks, as well as long term ergonomic interventions targeted for specific high risk tasks.
Two examples of high risk jobs in construction that require targeted interventions for awkward posture work are concrete rebar tiers and carpet layers. Frequent and prolonged stooping by concrete reinforcement workers (rodmen) is linked to a very high incidence of back pain in these workers. Targeted engineering controls for this job have the potential to eliminate the need for a stooped posture and consist of an automated extended-handle rebar tying tool and a device to store rebar at waist height. A field study of the use of rebar tying machines showed that they increased productivity, and significantly reduced the amount and duration of trunk flexion. The study also revealed that the use of this extended handle approach is not limited to reinforcing steel, but can be applied to other tasks, such as tying electrical conduit and attaching radiant heat tube to steel mesh (Vi, 2003). Resistance to the introduction of these tools has been based on early mechanical problems, limitations in the gauge of wire that can be handled, and concern on the part of ironworkers with the “de-skilling” of their profession.
Knee disorders in carpet layers are a well documented problem in this branch of the carpentry trade and are caused by prolonged kneeling and the use of a “knee kicker” device to stretch the newly laid carpet. Interventions for carpet layers address the problem by: 1) reducing the contact pressure on the knee with the use of overalls with knee pad pockets or knee pads in conjunction with a spring seat to support the weight of the body; 2) eliminating the use of the knee-kicker device by using a mechanical power stretcher; and 3) using tool extensions such as long-handled carpet cutting tools. Unfortunately, none of these interventions is optimal, and the kneeling-related knee problems of carpet layers remain a concern.
Manual materials handling (MMH) in construction often leads to prolonged stooping. A Dutch intervention study of bricklaying showed that the use of a crane to transport bricks and the use of height-adjustable scaffolding each resulted in dramatic reductions in the duration of extreme trunk flexion (van der Molen et al., 2004). These results are important given biomechanical research showing that manual materials handling at low working heights places the spine at increased risk for injury. Lifting and lowering materials at the bottom tier (level) of the pallet nearly doubles the compressive force on the spine compared with the middle and higher levels of the pallet (Gallagher, 1988). Height adjustable pallet handling equipment, which can be raised as the pallet is unloaded, can result in a significant reduction in spinal load by keeping the point of operation near waist height. In construction, this can be done by periodically lowering the forks of a lift truck if one is available at the time the materials are off-loaded.
Often in construction work, the problem of stooped or squatting postures is addressed by giving workers knee pads so they can perform the work while kneeling. However the injury prevention capabilities of knee pads are questionable. They do not mitigate the risks of extreme flexion, although they may help with pre-patellar bursitis. The benefits of knee pads are more clear with respect to acute injuries: preventing lacerations and penetrating injuries, as well as improving comfort by reducing contact stresses. There are many different types of knee pads available, and the selection of proper knee pads depends on the surface(s) being worked on and the frequency and type of movement. Although knee pads address some of the discomforts of kneeling work, one must be aware of the long term elevated LBD risk and knee disorder risk of working in the kneeling posture.
Although not discussed in detail in this Conference, research has been conducted on interventions for stooped postures in mining work. Ergonomics issues in mining are one of the research areas of the NIOSH mine safety program. The published research on ergonomic interventions for stooped and kneeling work in mining has focused on setting maximum acceptable weights of lift (MAWL) for combined lifting and lowering tasks in restricted height conditions, as well as improvements to tools and the way that they are used in the mine environment. The NIOSH Mining Safety website (
http://www.cdc.gov/niosh/mining) provides a collection of Mining Safety Tips that are an excellent resource for ergonomic intervention ideas to reduce MSD and LBD risk in mining. The ideas presented on this site come from miners, mining safety professionals, and NIOSH research, and are a testament to the collaborative efforts needed in ergonomic intervention development.
At the end of the conference, participants were asked to suggest where this dialogue and the effort to define, better understand and prevent work-related exposures to stooped, squatting and kneeling postures should go next.
SUGGESTIONS FOR ASSESSING HIGH RISK JOBS
- Evaluate the effectiveness of different methods of risk assessment with attention to predictive ability and field utility.
SUGGESTIONS FOR SURVEILLANCE RESEARCH
- Develop a national registry of musculoskeletal hazards and health outcomes.
- Add supplements to existing surveillance systems for stooped and kneeling postures.
- Conduct surveys in high risk industries (agriculture, construction, mining).
- Determine the number of workers exposed and what jobs they are doing.
- Record the exposure in identified jobs: time in stooped and squatting, by ‘zones’ of mild, moderate, and severe positions.
- Identify the specific job or task elements requiring stooped postures, and why.
- Conduct cross-sectional and longitudinal studies to develop and validate a list of high risk jobs and significant health outcomes.
SUGGESTIONS FOR INTERVENTION RESEARCH
- Develop new partnerships with agencies, academia and industry to support intervention research focused on stooped and kneeling work, including national and
regional partnerships focused on industry- or task specific applications.
- Increase the number and range of intervention research underway.
- Encourage higher-quality intervention evaluations using randomized trials, quasi-experimental designs and blended evaluations.
- Document and broaden the dissemination of successful/proven interventions.
SUGGESTIONS FOR ETIOLOGICAL RESEARCH
- Conduct studies to improve understanding of specific biomechanical stresses and MSD development during stooped and kneeling postures.
- Develop and evaluate improved standards and methods for assessing exposure, health outcomes and other etiological factors for stooped and kneeling work.
- Conduct population, clinical and laboratory studies to evaluate the short-term impacts of different types of exposure to working in stooped or kneeling postures on WMSD development and early indicators of such disorders.
- Conduct population, clinical and laboratory studies to evaluate the long-term impacts of different types of exposure to working in stooped or kneeling postures on WMSD development and early indicators of such disorders.
|
Anderson, J.A., E.O. Otun, and B.J. Sweetman. 1987. Occupational hazards and low back pain. Rev Environ Health 7:121-60.
Anderson JJ, Felson DT. 1988. Factors associated with osteoarthritis of the knee in the first national Health and Nutrition Examination Survey (HANES I). Evidence for an association with overweight, race, and physical demands of work. Am J Epidemiol 128:179-189.
Baker, P., I. Reading, C. Cooper, and D. Coggon. 2003. Knee disorders in the general population and their relation to occupation. Occup Environ Med 60:794-7.
Barrett, A. and F. A. Fathallah. 2001. Evaluation of four weight transfer devices for reducing loads on the lower back during agricultural stoop labor. American Society of Agricultural Engineers Paper Number 01-8056.
BLS. 2004. Occupational Outlook Handbook. 2004-05 ed. U.S. Department of Labor, Bureau of Labor Statistics, Bulletin 2570, Washington, D.C.
Burdorf, A., G. Govaert, and L. Elders. 1991. Postural load and back pain of workers in the manufacturing of prefabricated concrete elements. Ergonomics 34:909-18.
Cooper C, McAlindon T, Coggon D, Egger P, Dieppe P. 1994. Occupational activity and osteoarthritis of the knee. Ann Rheum Dis 53:90-93.
De and Sen 1986. J Human Ergol. 15; 103-112
Dimov M, Bhattacharya A, Lemasters G, Atterbury M, Greathouse L, Ollila-Glenn N. 2000. Exertion and body discomfort perceived symptoms associated with carpentry tasks: an on-site evaluation. AIHAJ 61:685-691.
Estill, C.F., and S. Tanaka. 1998. Ergonomic Considerations of Manually Harvesting Maine Wild Blueberries. Journal of Agricultural Safety and Health 4:43- 57.
Faucett, J., J. Meyers, J. Miles, I. Janowitz, and F. A. Fathallah. 2006. Rest break interventions in stoop labor tasks. Applied Ergonomics. Accepted for publication.
Felson DT, Hannan MT, Naimark A, Berkeley J, Gordon G, Wilson PW, Anderson J. 1991. Occupational physical demands, knee bending, and knee osteoarthritis: results from the Framingham Study. J Rheumatol 18:1587- 1592.
Felson DT, Radin EL. 1994. What causes knee osteoarthrosis: are different compartments susceptible to different risk factors? J Rheumatol 21:181-183.
Friedrich, M., T. Cermak, and I. Heiller. 2000. Spinal troubles in sewage workers: epidemiological data and work disability due to low back pain. Int Arch Occup Environ Health 73:245-54.
Galinsky, T.L., Swanson, N.G., Sauter, S.L., Hurrell, J.J., Schleifer, L.M. (2000). A field study of supplementary rest breaks for data-entry operators. Ergonomics. 43 (5), 622-638.
Gallagher, S., and C.A. Hamrick. 1992. Acceptable workloads for three common mining materials. Ergonomics 35:1013-31.
Gallagher S, Marras WS, Litsky AS, and Burr D., Torso flexion loads and the fatigue failure of human lumbosacral motion segments. Spine, 2005 Oct 15;30(20):2265-73.
Gallagher, S., W.S. Marras, K.G. Davis, and K. Kovacs. 2002. Effects of posture on dynamic back loading during a cable lifting task. Ergonomics 45:380-98.
Genaidy, A., Delgado, E., Bustos, T. 1995. Active microbreak effects on musculoskeletal comfort ratings in meatpacking plants, Ergonomics. 38(2):326-336.
Gite, LP. 1991. Optimum handle height for animal drawn mould board plough. Appl Ergon 22:21-28.
Granata KP, Rogers E, Moorhouse K, Effects of static flexion-relaxation on paraspinal reflex behavior. Clin Biomech (Bristol, Avon). 2005 Jan; 20(1):16-24.
Hannan MT, Felson DT, Anderson JJ, Naimark A. 1993. Habitual physical activity is not associated with knee osteoarthritis: the Framingham Study. J Rheumatol 20:704- 709.
Henning, R., Jaques, P., Kissel, G., Sullivan A., Alteras- Webb, S.1997. Frequent short rest breaks from computer work: Effects on productivity and well-being at two field sites. Ergonomics. 40(1):78-91.
Holmstrom, E.B., J. Lindell, and U. Moritz. 1992. Low back and neck/shoulder pain in construction workers: occupational workload and psychosocial risk factors. Part 1: Relationship to low back pain. Spine 17:663-71.
Hunting KL, Welch LS, Cuccherini BA, Seiger LA. 1994. Musculoskeletal symptoms among electricians. Am J Ind Med 25:149-163.
Hurwitz DE, Andriacchi TP. 1997. Biomechanics of the Hip and Knee. In: Nordin M, Andersson GBJ, editors. Musculoskeletal Disorders in the Workplace: Principles and Practice. Baltimore: Mosby.p 487-496.Janaro, R.E. and S.E. Bechtold. (1985) A study of the reduction of fatigue impact on productivity through optimal rest break scheduling, Human Factors, 27 (4), 459-466.
Janowitz, I., J.M. Meyers, D.G. Tejeda, J.A. Miles, V. Duraj, J. Faucett, and J.N. Kabashima. 1998. Reducing Risk Factors for the Development of Work-Related Musculoskeletal Problems in Nursery Work. Applied Occupational and Environmental Hygiene, 13:9-14.
Jensen LK, Eenberg W. 1996. Occupation as a risk factor for knee disorders. Scand J Work Environ Health 22:165- 175.
Jensen LK, Mikkelsen S, Loft IP, Eenberg W, Bergmann I, Logager V. 2000. Radiographic knee osteoarthritis in floorlayers and carpenters. Scand J Work Environ Health 26:257-262.
Keogh JP, Gucer PW, Gordon JL, Nuwayhid I. 2000. Patterns and predictors of employer risk-reduction activities (ERRAs) in response to a work-related upper extremity cumulative trauma disorder (UECTD): reports from workers’ compensation claimants. Am J Ind Med 38:489-497.
Kivimaki J. 1992. Occupationally related ultrasonic findings in carpet and floor layers’ knees. Scand J Work Environ Health 18:400-402.
Kivimaki J, Riihimaki H, Hanninen K. 1992. Knee disorders in carpet and floor layers and painters. Scand J Work Environ Health 18:310-316.
Kivimaki J, Riihimaki H, Hanninen K. 1994. Knee disorders in carpet and floor layers and painters. Part II: Knee symptoms and patellofemoral indices. Scand J Rehabil Med 26:97-101.
Kivimaki J, Riihimaki H, Alaranta H. 1994. Knee disorders in carpet and floor layers and painters. Part I. Isometric knee extension and flexion torques. Scand J Rehabil Med 26:91-95.
Kivimaki J, Hanninen K, Kujala UM, Osterman K, Riihimaki H. 1994. Knee laxity in carpet and floor layers and painters. Ann Chir Gynaecol 83:229-233.
Kleisinger, S. 2000. Ergonomic implications and technical solutions of the prone working position in horticulture. Proceedings of the IEA 2000/HFES 2000 Congress, San Diego, July 30 – Aug. 4, 2000.
Kohatsu ND, Schurman DJ. 1990. Risk factors for the development of osteoarthrosis of the knee. Clin Orthop 242- 246.
Konz, S (1998). Work/rest: Part I - Guidelines for the practitioner. International Journal of Industrial Ergonomics, 22: 67-71, 73-99.
Konz, S. 1998. Work/rest: Part I - Guidelines for the practitioner, pp. 67-71 International Journal of Industrial Ergonomics, Vol. 22.
Kumar, A., M. Varghese, D. Mohan, P. Mahajan, P. Gulati, and S. Kale. 1999. Effect of whole-body vibration on the low back. A study of tractor-driving farmers in north India. Spine 24:2506-15.
Lavender SA, Andersson GBJ. 1997. Job Accommodation with Respect to the Lower Extremity. In: Nordin M, Andersson GBJ, editors. Musculoskeletal Disorders in the Workplace: Principles and Practice. Baltimore: Mosby.p 528- 534.
Leigh, J.P., S.B. Markowitz, M. Fahs, C. Shin, and P.J. Landrigan. 1997. Occupational injury and illness in the United States. Estimates of costs, morbidity, and mortality. Arch Intern Med 157:1557-68.
Lemasters GK, Atterbury MR, Booth-Jones AD, Bhattacharya A, Ollila-Glenn N, Forrester C, Forst L. 1998. Prevalence of work related musculoskeletal disorders in active union carpenters. Occup Environ Med 55:421-427.
Lipscomb HJ, Dement JM, Gaal JS, Cameron W, McDougall V. 2000. Work-related injuries in drywall installation. Appl Occup Environ Hyg 15:794-802.
Marras, W.S., S.A. Lavender, S.E. Leurgans, F.A. Fathallah, S.A. Ferguson, W.G. Allread, and S.L. Rajulu. 1995. Biomechanical risk factors for occupationally related low back disorders. Ergonomics 38:377-410.
Marshall, R.N., and A.F. Burnett. 2004. A kinematic, kinetic and electromyographic comparison of stooped sheep shearing techniques and shearing with a sheep manipulator. Appl Ergon 35:137-45.
Mattila, T, Muuttomaa, E, Peltonen, M. 2001. The development of strawberry picking methods. In: (ed.) Clas- Håkan Nygård et al. Proceedings of NES 2001 Promotion of Health through Ergonomic Working and Living Conditions: Outcomes and methods of research and practise: publications 7. p. 464-466.
Merlino, L.A., J.C. Rosecrance, D. Anton, and T.M. Cook. 2003. Symptoms of musculoskeletal disorders among apprentice construction workers. Appl Occup Environ Hyg 18:57-64.
Meyer R. 2004. Research and Recent Ergonomic Developments in Prone Posture Workstations for Agriculture. American Society of Agricultural and Biological Engineers Annual Meeting, 2004.
Meyers, J., J. Miles, J. Faucett, I. Janowitz, D Tejeda, J. Kabashima. 1997. Ergonomics in Agriculture: Workplace Priority Setting in the Nursery Industry. American Industrial Hygiene Association Journal. 58(2):121-126
Meyers, J. M., J. A. Miles, J. Faucett, F. A. Fathallah, I. Janowitz, R. Smith, and E. Weber. 2006. Smaller loads reduce risk of back injuries during wine grape harvest. California Agriculture 60 (1):25-31.
Meyers, J.M., J.A. Miles, J. Faucett, I. Janowitz, D.G. Tejeda, E. Weber, R. Smith, and L. Garcia. 2001. Priority Risk Factors for Back Injury in Agricultural Field Work: Vineyard Ergonomics. Journal of Agromedicine 8:37-52.
Morse T, et al, Capture-Recapture Estimation of Unreported Work-Related Musculoskeletal Disorders in Connecticut, American Journal of Industrial Medicine, 39: 636-642, 2001.
Myllymaki T, Tikkakoski T, Typpo T, Kivimaki J, Suramo I. 1993. Carpet-layer‘s knee. An ultrasonographic study. Acta Radiol 34:496-499.
Nag, PK and CK Pradhan. 1992. Ergonomics in the hoeing operation. Int J Ind Erg 10:341-350.
Nag, PK, NC Sebastian, and MG Marlankar. 1980. Occupational workload of Indian agricultural workers. Ergonomics 23:91-102.
Nag, PK, A Goswami, SP Ashtekar, and CK Pradhan. 1988. Ergonomics in sickle operation. Appl Ergon 19:233- 239.
Nag et al. 1992. Int J Ind Ergonomics 10(4)341-350
Nagura T, Dyrby CO, Alexander EJ, Andriacchi TP. 2002. Mechanical loads at the knee joint during deep flexion. J Orthop Res 20:881-886.
Nakagawa S, Kadoya Y, Kobayashi A, Tatsumi I, Nishida N, Yamano Y. 2003. Kinematics of the patella in deep flexion. Analysis with magnetic resonance imaging. J Bone Joint Surg Am 85-A:1238-1242.
National Research Council and Institute of Medicine. 2001. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities, In P. o. M. D. a. t. Workplace., (ed.) Commission on Behavioral and Social Sciences and Education. National Academy Press, Washington, D.C.
NIOSH. 1997. Musculoskeletal Disorders and Workplace Factors: A Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back, In B. P. Bernard, ed. U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) No. 97-141, Cincinnati, OH.
Olson, M.W., L. Li, and M. Solomonow. 2004. Flexionrelaxation response to cyclic lumbar flexion. Clin Biomech (Bristol, Avon) 19:769-76.
Punnett, L., L.J. Fine, W.M. Keyserling, G.D. Herrin, and D.B.
Paquet VL, Punnett L, Buchholz B. 2001. Validity of fixed-interval observations for postural assessment in construction work Appl Ergon 32:215-224. Chaffin. 1991. Back disorders and nonneutral trunk postures of automobile assembly workers. Scand J Work Environ Health 17:337-46.
Paskeiweicz, J., and F. A. Fathallah. 2006. Effectiveness of a manual furniture handling device in reducing low back disorders risk factors. International Journal of Industrial Ergonomics. Accepted for publication.
Ramazzini, B. 1713. De Morbis Artificum Diatriba (Diseases of Workers). Latin 1713 second edition ed. University of Chicago Press, Chicago.
Rullmann M, Kleisinger, S. 2003. Ergonomics investigations in the prone working posture during pickling cucumber harvesting. XXX CIOSTA CIGR V Management and technology applications to empower agriculture and agrofood systems, 22-24 September 2003 University of Turin, Turin, Italy.
Solomonow, M., R.V. Baratta, A. Banks, C. Freudenberger, and B.H. Zhou. 2003. Flexion-relaxation response to static lumbar flexion in males and females. Clin Biomech (Bristol, Avon) 18:273-9.
Spanu CE, Hefzy MS. 2003. Biomechanics of the knee joint in deep flexion: a prelude to a total knee replacement that allows for maximum flexion. Technol Health Care 11:161-181.
Spielholz P, Wiker SF, Silverstein B. 1998. An ergonomic characterization of work in concrete form construction. Am Ind Hyg Assoc J 59:629-635.
Van Der Molen, HF, Grouwstra, R, Kuijer, PPFM, Sluiter, JSK, Frings-Dresen, MHW. 2004. Efficacy of adjusting working height and mechanizing of transport on physical work demands and local discomfort in construction work, Ergonomics, 47:7, 772 – 783.
Vi, Peter (2003), “Reducing Risk of Musculoskeletal Disorders through the Use of Rebar Tying Machines.” Applied Occupational and Environmental Hygiene 18:1-6.
Welch LS, Hunting KL, Nessel-Stephens L. 1999. Chronic symptoms in construction workers treated for musculoskeletal injuries. Am J Ind Med 36:532-540.
Wickstrom G, Hanninen K, Mattsson T, Niskanen T, Riihimaki H, Waris P, Zitting A. 1983. Knee degeneration in concrete reinforcement workers. Brit J Ind Med 40:216-219.
This conference could not have been held without the active support of the National Institute for Occupational Safety and Health. NIOSH supported the conference financially with Conference Grant CDC C13/CCC923627- 01. Dr. Sean Gallagher of NIOSH presented at the conference. Dr. Tom Waters of NIOSH provided advice, assistance and presented at the conference.
The conference is also indebted to Dr. Laura Welch and the Center to Protect Workers Rights and to Ms. R. J. Banks and the State Compensation Insurance Fund of California for co-sponsoring and actively participating.
The staff of the UC Center for Occupational and Environmental Health deserve our special thanks for allowing the conference to be part of the Center’s annual Summer Institute and for providing all administrative support.
The faculty, students and staff of the UC Agricultural Ergonomics Research Center provided the impetus for the conference and provided core planning leadership and much of the academic support. A special thank you to Brandon Miller for his invaluable contribution to these proceedings.
Fadi A. Fathallah, PhD, AEP
Associate Professor
Biological and Agricultural Engineering
University of California Davis
One Shields Avenue
Davis, CA 95616
530-752-1612 Fax: 530-752-2640
fathallah@ucdavis.edu
James M. Meyers, EdD, MPH
Agricultural Health & Safety Specialist
School of Public Health
University of California Berkeley
140 Warren Hall, Mailcode 7360
Berkeley, CA 94720-7360
510-643-5310 Fax: 510-642-5815
jmmeyers@berkeley.edu
Ira Janowitz, MS, PT, CPE
Senior Ergonomics Consultant
University of California Ergonomics Program
1301 South 46th Street, #163
Richmond, CA 94804
(925) 351-1142 Fax: (510) 665-3423
janowitz@comcast.net
John A. Miles, PhD
Professor
Biological and Agricultural Engineering
University of California Davis
3052 Bainer Hall
Davis, CA 95616
530-754-8817 Fax: 530-752-2640
jamiles@ucdavis.edu
R.J. Banks, MS, CIE
Ergonomics Services Supervisor
State Compensation Insurance Fund
303 Second Street, Suite 205
South San Francisco, CA 94107-1329
415-975-2401
Fax: 415-975-2444
rjbanks@scif.com
Julia Faucett, RN, PhD, FAAN
Professor and Chair
Dept of Community Health Systems
UCSF School of Nursing
Box 0608
San Francisco, CA 94143-0608
415-475-3221
Fax: 415-476-6042
julia.faucett@nursing.ucsf.edu
Sean Gallagher, PhD, CPE
Physiologist
NIOSH
626 Cochrans Mill Road
Pittsburgh, PA 15236
412-386-6445
Fax: 412-386-5108
sfg@cdc.gov
Willette “Billy” Gibbons
President (1994-2007)
DGI Ergonomics & Safety
Leadership Services
4520 18th Place South
Salem, OR 97302
503-581-8560
Fax: 503-581-1410
Adarsh Kumar, PhD
Senior Scientist
Indian Agricultural Research Institute
Division of Agricultural Engineering
IARI
New Delhi 110012 India
Tel: 0091-11-25842294
Fax: 0091-11-26858703
adarsh_iari@rediffmail.com
Peter Lundqvist, PhD
Professor
Division of Work Science
Agricultural Biosystems and
Technology
Swedish University of Agricultural
Sciences
Box 88 (Sundsvagen 1)
Alnarp S23053 Sweden
01146-40 415495
Fax: 01146-40 415489
Peter.Lundqvist@jbt.slu.se
Robert H. Meyer, MS
Biomedical Engineering Department
1550 Engineering Drive, Room 2157
Madison, WI 53706
608-262-8455 (phone)
rhmeyer1@wisc.edu
William S. Marras, PhD
Professor
College of Engineering
Ohio State University
1971 Neil Avenue
Columbus, OH 43210
614-292-6670
marras.1@osu.edu
Suzanne H. Rodgers, PhD
Consultant in Ergonomics
169 Huntington Hills
Rochester, NY 14622
Phone/Fax: 585-544-3587
SHRODGERS@aol.com
John Rosecrance, PhD, CPE
Professor
Colorado State University
1681 Campus Delivery
Fort Collins, CO 80523
970-491-1405
john.rosecrance@colostate.edu
Thomas R. Waters, PhD, CPE
Leader,
Human Factors & Ergonomics Group
NIOSH
4676 Columbia Parkway
Cincinnati, OH 45226
513-533-8147
Fax: 513-533-8596
trw1@cdc.gov
Laura S. Welch, MD
Medical Director
Center to Protect Workers’ Rights
8484 Georgia Avenue, Suite 1000
Silver Spring, MD 20910
301-495-8505
Fax: 301-578-8572
lwelch@cpwr.com
Disclaimer and Reproduction Information: Information in
NASD does not represent NIOSH policy. Information included in
NASD appears by permission of the author and/or copyright holder.
More