SUMMARY
In winter 2012, a male farm hand in his 60s died when he was struck by a 2006 Komatso WA 250 front end loader with an 8-foot 10-inch wide, 4-cubic yard bucket. The incident occurred prior to sunrise. The weather was overcast with little moonlight. The decedent had traveled to the area with a skid steer loader and positioned the loader so its lights partially illuminated his work area. He was wearing dark clothes and a dark hat. An 18-foot “driveway” was between a bunker silo and the 300-foot-long silage pile where the decedent was bent over cutting the strings to open a hay bale. In the area where the decedent was working, the silage protruded approximately seven feet, which placed the decedent in the shadows. The front end loader operator was rounding the corner of the bunker silo on his way to obtain additional feed. It is hypothesized that the corner of the front end loader bucket struck the decedent. The impact knocked the decedent to the ground and he was run over by the front left loader tire (Figure 1). The decedent was alert and breathing when transported by helicopter to a nearby hospital. He died the following day from complications of the injuries sustained at the time of the incident.
Contributing Factors
RECOMMENDATIONS
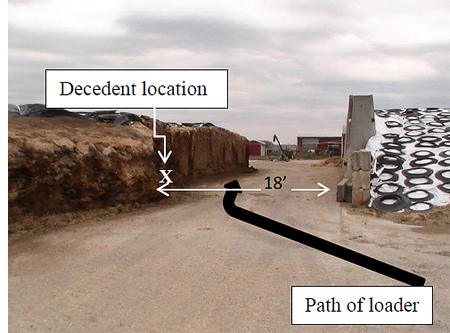
Figure 1. Incident area showing decedent’s location
and
travel path of loader
In winter 2012, a male farm hand in his 60s died when he was struck by a 2006 Komatso WA 250 front end loader with an 8-foot 10-inch wide, 4-cubic yard bucket. MIFACE learned of this incident from the MIOSHA 24-hour hotline. MIFACE contacted the farm owner, who agreed to participate in the MIFACE research program. MIFACE personnel visited the farm and interviewed the farm owner who was also the brother of the decedent. The farm owner escorted the researchers to the incident site and gave permission to the MIFACE researcher to take pictures of the incident scene. During the writing of this report, MIFACE reviewed the MIOSHA compliance investigation file, the death certificate and the police report and pictures.
The 700-head dairy farm was a family-owned operation. The farm operation also grew corn, soybeans, wheat, and alfalfa on 2,000 acres. The decedent was a contractual employee. The farm employed 14 full-time workers and four part-time workers. The decedent worked full time. He had worked on the farm for the past eight years, but had worked periodically for the farm throughout his working lifetime. His work hours at the farm were 5:00 a.m. to 3:30 p.m.
The farm owner had a safety training program but did not have a written safety program. All new employees were required to attend a new employee safety orientation. Employee training documentation was not maintained. Additionally, animal handler training and skid steer loader training was conducted. Every fall and spring, the farm offered fatigue awareness. Safety rules, such as prohibiting work in an area where a front end loader was operating were in place. The safety rules were communicated verbally; the rules were not documented.
The decedent was described as a worker who always needed to be active when on the farm. The decedent and all of the farm employees have been instructed not to be near the wheel loader or the feed pile while the loader is being operated.

Figure 2. Location of high lumen sodium light.
The farm owners instituted the following work practice changes to prevent a similar incident:
MIOSHA General Industry Safety and Health Division did not find a violation of a General Industry Safety or Health Standard. The Division issued two Safety and Health Recommendations at the conclusion of its investigation:

Figure 3. Bunker configuration change - note
angle of cement compared to Figure 1 and
approximate location of decedent.
The incident occurred prior to dawn. The incident scene was an unlit, flat, frozen muddy 18-foot wide “driveway” area. A 300-foot long silage pile was located on the north side of the driveway. On the south side of the silage pile were some hay bales bound by strings.
Across from and to the south of the silage pile was a bunker silo with an east and west section. The feed mixer and tractor was facing west and was located to the south of the silage pile and the west bunker silo.
A 2006 Komatso WA 250 front end loader weighing approximately 10,700 pounds with a 4-cubic yard bucket measuring 8 feet, 10 inches in width was operated by a farm employee to transport feed from the east bunker silo to the feed mixer. The wheel loader’s lights were functioning properly and were on at the time of the incident. The front end loader operator, who had started work at 4:00 a.m., passed through the area several times to unload feed into the feed mixer, which was located by a commodity shed.
The decedent had traveled to the area with a skid steer loader. He positioned the loader so its lights could partially illuminate his work area. The decedent was wearing dark clothing and a dark hat. In the area where he was cutting open the bales of hay, which was used for bedding for the cows. In this area, the silage protruded approximately seven feet, placing the decedent in the shadows. The area where he was working was near the end of the west bunker silo.
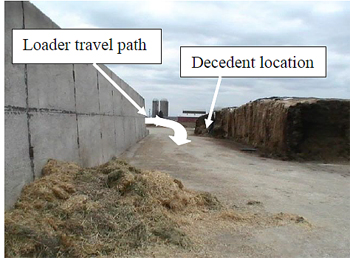
Figure 4. Incident area, standing on east end
of bunker silo looking west.
With the front end loader facing south, the operator unloaded the contents of the bucket of the loader. The operator then backed up while turning the rear of the loader to the west so that the loader faced east. He then drove forward and began to round the corner of the bunker silo (Figure 4). He did not know that the decedent was working in the area.
The front end loader operator did not see the decedent because of the dark and dusty conditions and because decedent was on the ground on foot in dark clothing. Both the police and the farm owner hypothesized that the decedent was struck by the loader bucket and then run over by the left front wheel of the loader while the operator was driving forward.
The driver felt a bump on the left front tire. He immediately stopped the wheel loader. He exited and saw that the decedent had been struck and run over. The decedent was positioned between the loader’s front and back tires. When police arrived, the decedent was alert, conscious and breathing. The decedent sustained injuries on the left side of his body.
Prior to being airlifted to a local hospital, the decedent stated to the responding fire department personnel “It’s not his fault – I shouldn’t have been there.” He died the next day from injuries sustained in incident.
The cause of death as listed on the death certificate was multiple blunt force injuries. An autopsy was not performed.

Figure 5. Possible signage location
MIFACE recommends the farm owners evaluate all farm activities to evaluate work practices necessary to perform them safely. Certain tasks, currently being performed at during the night (or in the dark) may be able to be performed partially during daylight hours to reduce night operation risks.
The farm has established the area where the incident occurred as a restricted work area - restricting personnel access when it is dark. Although training had been performed, a sign/pictogram could be placed on the bunker walls (Figure 5) warning workers of the danger in the area and of the restricted nature of the area to serve as a visual reminder. Because the farm had workers who spoke Spanish, MIFACE recommends posting this area with a pictogram or sign in both English and Spanish as a reminder to workers.
A significant amount of work on a dairy farm is performed during non-daylight hours. Additional lighting on the loader (Figure 6) and the skid steer would increase the visibility of workers on foot as well as providing the machine operators better visibility for equipment operation.

Illustration 1. Example of pictogram to alert workers.
The new feed mixer location is not located in a well-lit area. MIFACE recommends that the farm owner assess the lighting in this area and consider the installation of a high lumen sodium yard light.
High visibility clothing is a type of personal protective equipment with highly reflective properties or is a color that is easily discernible from any background. The farm now requires workers to wear high visibility vests during non-daylight hours. MIFACE recommends that the farm consider the use of additional visibility options for workers on foot, such as high visibility or “loud color” ball caps or utilize a bicycle-type strobe light that could be attached to a piece of clothing or to a ball cap. MIFACE recommends that the farm owners require the additional visibility options to be worn at all times, including the daylight hours, while on foot in equipment travel areas.

Figure 6. Front end loadter involved in incident.
Although not the same model number, the NIOSH Workplace Safety and Health Topic, Highway Work Zone Safety, Construction Equipment Visibility provided a ground level blind area diagram for the Komatsu WA 480. Illustration 1 shows the ground level diagram identifying the machine operator blind spots for objects at a 3-foot height (approximately the height of a construction barrel). The areas in grey show the areas that the machine operator cannot see. With the decedent bending over, he would have been less than three feet high and it would have been extremely difficult for the operator to see him.
Employers should use the blind spot diagrams provided by NIOSH to train both the work on foot and the machine operator to develop awareness about hazardous areas around construction vehicles and equipment due to limited visibility.
During conversation with the farm owner, a discussion about safe work practice checklists was held. The farm owner was questioning how he could “enforce” a consistent level of safe work activity among his English speaking and Spanish speaking employees. A checklist of acceptable and unacceptable work practices was suggested. Unacceptable work practices that may lead to serious injury and/or death could be identified and if an employee is noted to be engaging in those work practices, the employee is subject to immediate dismissal. An example of this could be the wearing of the high visibility vest during non-daylight hours. The expected safe work practice is to wear the vest. An unsafe work practice is not wearing the vest and is subject to disciplinary procedures. An example of an unsafe work practice subject to immediate dismissal is the employee in the restricted work area during non-daylight hours without the vest. The lists will assist in employee training efforts and provide consistent expectations for all workers and managers.
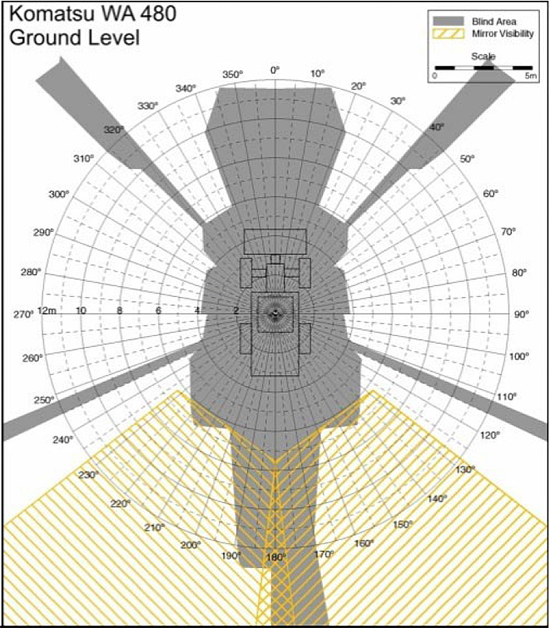
Illustration 1. NIOSH Construction Equipment Visibility Chart, Komatsu WA 480, ground level
National Institute for Occupational Safety and Health (NIOSH). Highway Work Zone Topic Page, Construction Equipment Visibility. http://www.cdc.gov/niosh/topics/highwayworkzones/BAD/imagelookup.html
My Safety Sign. http://www.mysafetysign.com.
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 909 Fee Road, 117 West Fee Hall, East Lansing, Michigan 48824-1315; http://www.oem.msu.edu. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer.
Publication #: #12MI008 | August 6, 2013
Disclaimer and Reproduction Information: Information in NASD does not represent NIOSH policy. Information included in NASD appears by permission of the author and/or copyright holder. More